Kim Han Jo, Nemani Venu, Boachie-Adjei Oheneba, Cunningham Matthew E, Iorio Justin A, O'Neill Kevin, Neuman Brian J, Lenke Lawrence G
Hospital for Special Surgery, Spine Care Institute, New York, NY, USA.
Vanderbilt University Medical Center, Nashville, TN, USA.
Global Spine J. 2017 May;7(3):254-259. doi: 10.1177/2192568217699183. Epub 2017 Apr 7.
Retrospective study.
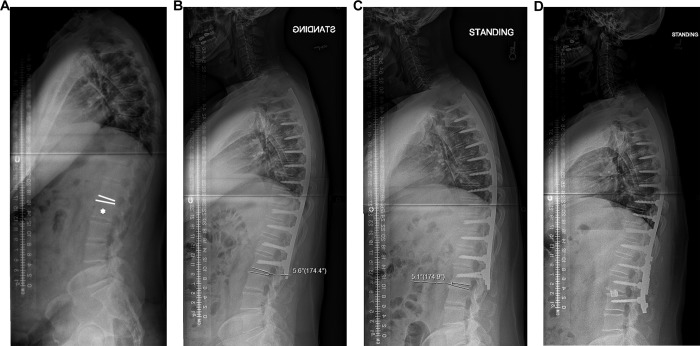
To compare 2 methods of selecting the lowest instrumented vertebra (LIV) on the rates of revision surgery for distal junctional kyphosis (DJK) following treatment for Scheuermann's kyphosis (SK).
A retrospective review of patients who have undergone surgical treatment for SK was performed. Forty-four patients were divided into 2 groups based on intervention: Group 1 (n = 26) included patients who had an LIV distal to or at the sagittal stable vertebrae (SSV), and Group 2 (n = 18) included patients who had an LIV proximal to the SSV. For each group, demographic, radiographic, and revision surgery data was analyzed.
The average follow-up was 3.1 years. There were no differences among demographic variables between the groups. Preoperative and postoperative thoracic kyphosis, lumbar lordosis, and sagittal balance were not different between groups. Postoperatively, Group 1 demonstrated a significantly greater average lordotic disc angle below the LIV compared with Group 2 (Group 1, -6.2 ± 4.3° vs Group 2, -2.9 ± 5.8°; = .02). In a subgroup analysis, extending fusions to the sagittal stable vertebra rather than the first lordotic disc resulted in fewer distal LIV complications necessitating revision surgery compared with fusing short of the SSV (5% vs 36.3%, = .04).
The SSV method may reduce complications secondary to distal junctional failure, but at the expense of incorporating additional motion segments in a typically young population.
回顾性研究。
比较两种选择最低融合椎体(LIV)的方法对Scheuermann驼背(SK)治疗后远端交界性后凸畸形(DJK)翻修手术发生率的影响。
对接受SK手术治疗的患者进行回顾性分析。根据干预措施将44例患者分为两组:第1组(n = 26)包括LIV位于矢状面稳定椎体(SSV)远端或与其平齐的患者,第2组(n = 18)包括LIV位于SSV近端的患者。对每组患者的人口统计学、影像学和翻修手术数据进行分析。
平均随访3.1年。两组间人口统计学变量无差异。两组术前和术后的胸椎后凸、腰椎前凸和矢状面平衡无差异。术后,第1组LIV下方的平均前凸椎间盘角度明显大于第2组(第1组,-6.2±4.3° vs 第2组,-2.9±5.8°;P = 0.02)。在亚组分析中,与融合至SSV以下相比,将融合范围扩展至矢状面稳定椎体而非第一个前凸椎间盘,导致需要翻修手术的远端LIV并发症更少(5% vs 36.3%,P = 0.04)。
SSV方法可能会减少远端交界性失败继发的并发症,但代价是在通常较年轻的人群中纳入了额外的运动节段。