Department of Epidemiology, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina.
Department of Medicine, University of North Carolina School of Medicine, Chapel Hill, North Carolina.
Diabetes Obes Metab. 2018 Jan;20(1):129-140. doi: 10.1111/dom.13049. Epub 2017 Aug 8.
To compare bladder cancer incidence between patients initiating pioglitazone treatment and patients initiating treatment with dipeptidyl-peptidase-4 inhibitors [DPP-4s] or sulfonylureas.
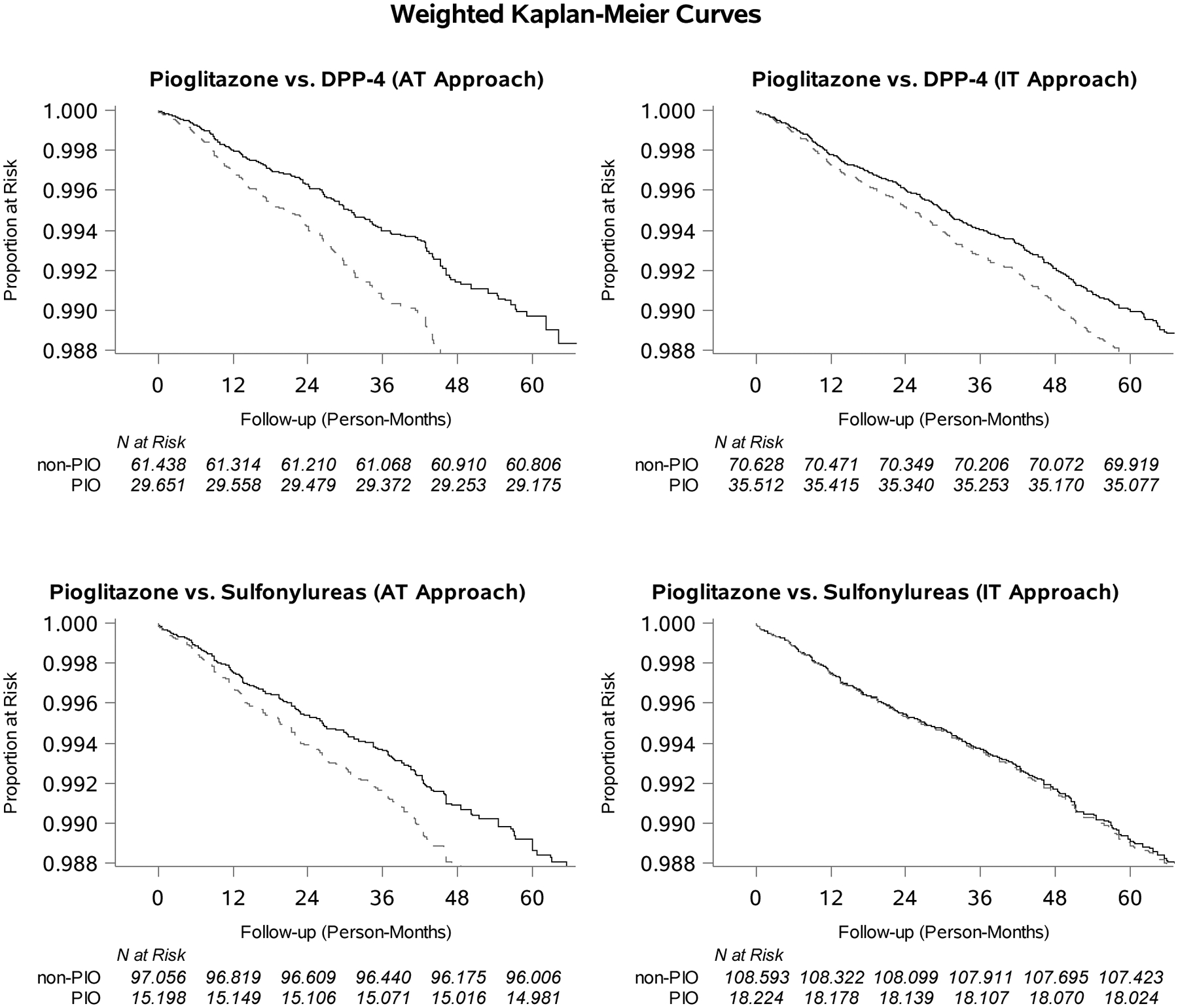
We identified Medicare beneficiaries aged >65 years who initiated treatment with pioglitazone (N = 38 700), DPP-4s (N = 82 552) or sulfonylureas (N = 126 104) between 2007 and 2014 after at least 6 months without prescriptions for these drug classes. Patients were followed from second prescription until bladder cancer outcome (2 claims within 60 days) using a 6-month induction/latency period, censoring for treatment change, death or end of 2014. We used propensity score-weighted Cox proportional-hazards models to obtain adjusted hazard ratios (aHR) and their 95% confidence intervals.
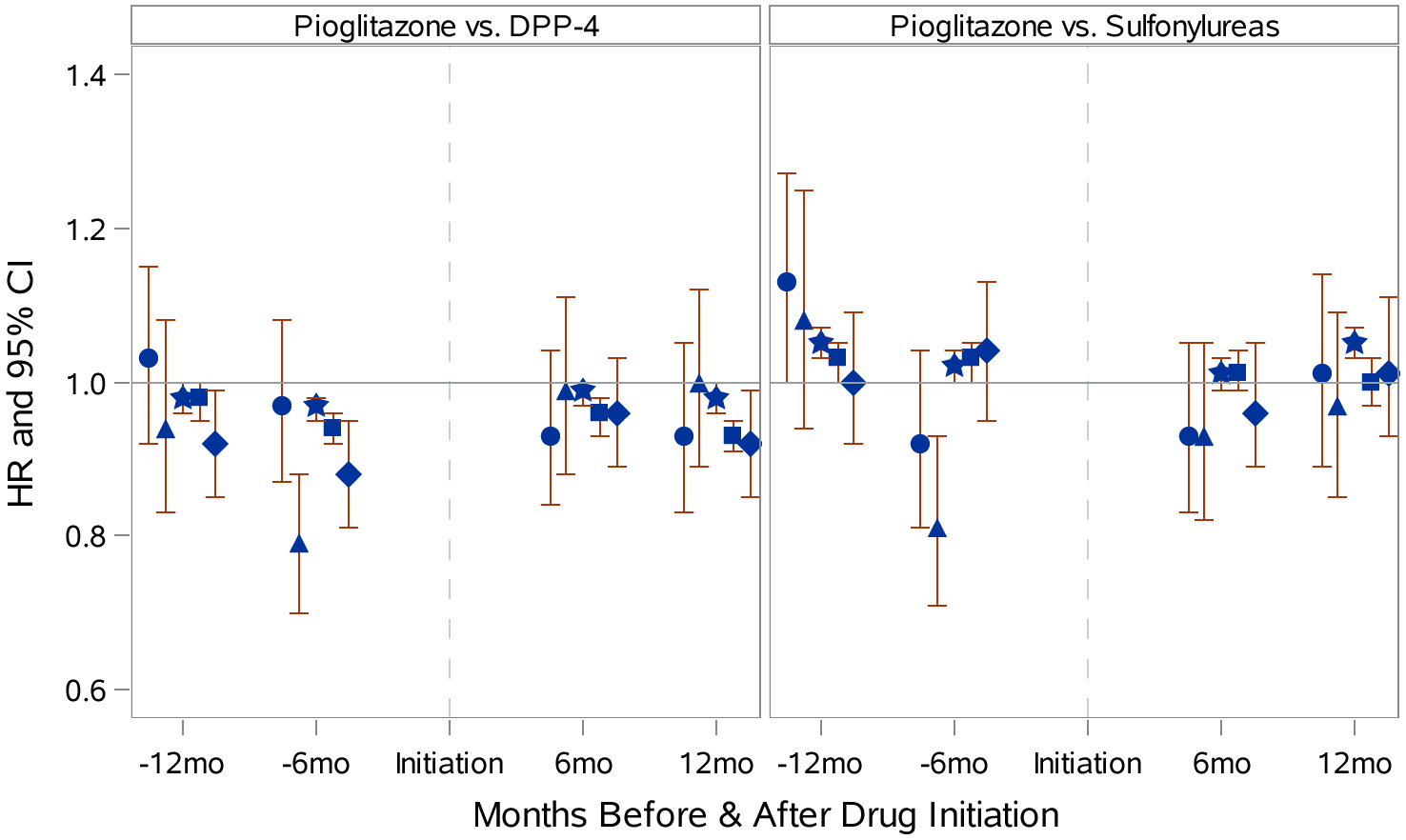
Overall mean age of participants was 75 years and 41% were men. Over a median of 1.2 treatment years, 727 beneficiaries developed bladder cancer. Pioglitazone initiators had an increased incidence of bladder cancer (308 vs 204 [DPP-4s] or 231 [sulfonylureas] per 100 000 person-years; aHR, 1.57 [1.23-2.00] vs DPP-4s and 1.32 [1.02-1.70] vs sulfonylureas). The increased risk emerged within the first 2 years of treatment (aHR, 1.63 [1.22-2.17] vs DPP-4s and 1.32 [0.98-1.78] vs sulfonylureas). If treatment was discontinued within the first 2 years, the risk after 2 years post initiation was attenuated (aHR, 0.89 [0.61-1.28]) compared with patients treated for more than 2 years (aHR, 1.45 [0.93-2.26]) both vs DPP-4s. Findings were consistent across secondary and sensitivity analyses.
Pioglitazone was associated with an elevated risk of bladder cancer compared with DPP-4s and sulfonylureas. The elevated risk emerged within the first 2 years of treatment and was attenuated after discontinuing. Pioglitazone's relative effectiveness should be weighed against a small absolute increase in risk of bladder cancer.
比较起始吡格列酮治疗与起始二肽基肽酶-4 抑制剂[DPP-4s]或磺酰脲类药物治疗的患者膀胱癌发病率。
我们确定了年龄>65 岁的 Medicare 受益人,他们在 2007 年至 2014 年期间至少在 6 个月内没有使用这些药物类别后开始接受吡格列酮(N=38700)、DPP-4s(N=82552)或磺酰脲类药物(N=126104)治疗。使用 6 个月的诱导/潜伏期(因治疗变更、死亡或 2014 年底结束而进行删失),从第二次处方开始,对患者进行随访,直到膀胱癌结局(60 天内的 2 次索赔)。我们使用倾向评分加权 Cox 比例风险模型获得调整后的风险比(aHR)及其 95%置信区间。
参与者的总体平均年龄为 75 岁,其中 41%为男性。在中位治疗时间为 1.2 年期间,有 727 名患者发生膀胱癌。吡格列酮治疗者膀胱癌发病率升高(308 例与 204 例[DPP-4s]或 231 例[磺酰脲类药物]每 100000 人年;aHR,1.57[1.23-2.00]与 DPP-4s 和 1.32[1.02-1.70]与磺酰脲类药物)。这种风险增加出现在治疗的前 2 年内(aHR,1.63[1.22-2.17]与 DPP-4s 和 1.32[0.98-1.78]与磺酰脲类药物)。如果在治疗的前 2 年内停药,则在开始治疗 2 年后的风险降低(aHR,0.89[0.61-1.28])与治疗超过 2 年的患者相比(aHR,1.45[0.93-2.26])均与 DPP-4s 相比。二次和敏感性分析结果一致。
与 DPP-4s 和磺酰脲类药物相比,吡格列酮与膀胱癌风险升高相关。这种风险出现在治疗的前 2 年内,停药后风险降低。吡格列酮的相对有效性应与膀胱癌风险的微小绝对增加相权衡。