Yu Amy Y X, Quan Hude, McRae Andrew D, Wagner Gabrielle O, Hill Michael D, Coutts Shelagh B
Department of Clinical Neurosciences, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada.
Department of Community Health Sciences, University of Calgary, Calgary, Alberta, Canada.
BMJ Open. 2017 Jul 2;7(6):e015234. doi: 10.1136/bmjopen-2016-015234.
Administrative health data are valuable in health research and disease surveillance, but have low to moderate sensitivity in identifying transient ischaemic attacks (TIA) in the emergency department (ED). We aimed to identify the predictors of coding accuracy for TIA.
The study population was obtained from two ongoing studies on the diagnosis of TIA, minor stroke and stroke mimic. ED charts were manually reviewed by a stroke neurologist to obtain the clinical diagnosis, patient characteristics and content of physician documentation. Administrative data codes were compared with the chart-adjudicated diagnosis to determine cases of misclassification by administrative data. Univariable regression was used to evaluate candidate predictors of disagreement, and the significant variables were tested in a multivariable model to obtain an adjusted estimate of effect.
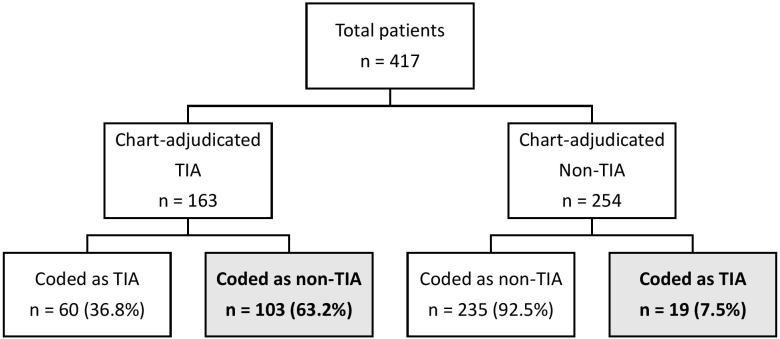
Among 417 patients (39.1% TIA, 37.2% minor stroke and 23.7% stroke mimics), there were 122 cases of disagreement between adjudications and administrative data codes for the diagnosis of TIA. The majority of disagreement (n=103/122, 84.4%) arose from adjudicated TIA cases that were misclassified as non-TIA in administrative data coding. There were 78 (18.7%) charts with documented uncertain diagnosis, and 73 (17.5%) charts had no definite diagnosis. The relative risk of disagreement between chart adjudication and administrative data coding when the final diagnosis was uncertain or absent was 1.82(1.36, 2.44) and the risk difference was 18.5%. Multivariable logistic regression analyses confirmed this association using different case definition algorithms.
In suspected patients with TIA and minor stroke presenting to the ED, physician documentation was the dominant factor in coding accuracy, supporting the concept that physicians are active participants in administrative data coding. Strategies to improve chart documentation are predicted to have a positive effect on coding accuracy.
行政卫生数据在健康研究和疾病监测中很有价值,但在急诊科(ED)识别短暂性脑缺血发作(TIA)方面的敏感性较低至中等。我们旨在确定TIA编码准确性的预测因素。
研究人群来自两项正在进行的关于TIA、轻度卒中及卒中样发作诊断的研究。由一名卒中神经科医生人工查阅ED病历,以获取临床诊断、患者特征和医生记录内容。将行政数据编码与经病历判定的诊断进行比较,以确定行政数据误分类的病例。采用单变量回归评估不一致的候选预测因素,并在多变量模型中对显著变量进行测试,以获得效应的调整估计值。
在417例患者中(39.1%为TIA,37.2%为轻度卒中,23.7%为卒中样发作),有122例经判定的诊断与行政数据编码在TIA诊断上存在不一致。大多数不一致情况(n=103/122,84.4%)源于经判定为TIA的病例在行政数据编码中被误分类为非TIA。有78份(18.7%)病历记录了不确定诊断,73份(17.5%)病历没有明确诊断。当最终诊断不确定或不存在时,病历判定与行政数据编码之间不一致的相对风险为1.82(1.36,2.44),风险差异为18.5%。多变量逻辑回归分析使用不同的病例定义算法证实了这种关联。
在就诊于ED的疑似TIA和轻度卒中患者中,医生记录是编码准确性的主要因素,支持了医生是行政数据编码积极参与者的概念。预计改善病历记录的策略将对编码准确性产生积极影响。