Lucie Thomassin, Laura Armengol-Debeir, Cloé Charpentier, Guillaume Savoye, Department of Gastroenterology, Rouen University Hospital, University of Rouen, F-76031 Rouen, France.
World J Gastroenterol. 2017 Jun 21;23(23):4285-4292. doi: 10.3748/wjg.v23.i23.4285.
To evaluate the imaging course of Crohn's disease (CD) patients with perianal fistulas on long-term maintenance anti-tumor necrosis factor (TNF)-α therapy and identify predictors of deep remission.
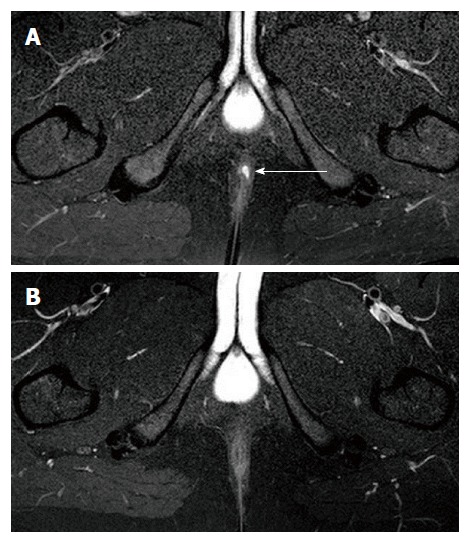
All patients with perianal CD treated with anti-TNF-α therapy at our tertiary care center were evaluated by magnetic resonance imaging (MRI) and clinical assessment. Two MR examinations were performed: at initiation of anti-TNF-α treatment and then at least 2 years after. Clinical assessment (remission, response and non-response) was based on Present's criteria. Rectoscopic patterns, MRI Van Assche score, and MRI fistula activity signs (T2 signal and contrast enhancement) were collected for the two MR examinations. Fistula healing was defined as the absence of T2 hyperintensity and contrast enhancement on MRI. Deep remission was defined as the association of both clinical remission, absence of anal canal ulcers and healing on MRI. Characteristics and imaging patterns of patients with and without deep remission were compared by univariate and multivariate analyses.
Forty-nine consecutive patients (31 females and 18 males) were included. They ranged in age from 14-70 years (mean, 33 years). MRI and clinical assessment were performed after a mean period of exposure to anti-TNF-α therapy of 40 ± 3.7 mo. Clinical remission, response and non-response were observed in 53.1%, 20.4%, and 26.5% of patients, respectively. Deep remission was observed in 32.7% of patients. Among the 26 patients in clinical remission, 10 had persisting inflammation of fistulas on MRI (T2 hyperintensity, = 7; contrast enhancement, = 10). Univariate analysis showed that deep remission was associated with the absence of rectal involvement and the absence of switch of anti-TNF-α treatment or surgery requirement. Multivariate analysis demonstrated that only the absence of rectal involvement (OR = 4.6; 95%CI: 1.03-20.5) was associated with deep remission.
Deep remission is achieved in approximately one third of patients on maintenance anti-TNF-α therapy. Absence of rectal involvement is predictive of deep remission.
评估长期维持抗肿瘤坏死因子(TNF)-α治疗的克罗恩病(CD)患者伴肛周瘘管的影像学过程,并确定深度缓解的预测因素。
我们对在三级医疗中心接受抗 TNF-α 治疗的所有肛周 CD 患者进行了磁共振成像(MRI)和临床评估。进行了两次 MRI 检查:在开始抗 TNF-α 治疗时,然后至少在 2 年后。临床评估(缓解、反应和无反应)基于 Present 标准。收集了两次 MRI 检查的直肠镜模式、MRI Van Assche 评分和 MRI 瘘管活动征象(T2 信号和对比增强)。MRI 定义瘘管愈合为无 T2 高信号和对比增强。深度缓解定义为临床缓解、肛门内无溃疡以及 MRI 愈合的联合存在。通过单变量和多变量分析比较有和无深度缓解患者的特征和影像学模式。
共纳入 49 例连续患者(31 名女性和 18 名男性),年龄 14-70 岁(平均 33 岁)。MRI 和临床评估在接受抗 TNF-α 治疗后平均 40 ± 3.7 个月进行。分别观察到 53.1%、20.4%和 26.5%的患者达到临床缓解、反应和无反应。32.7%的患者达到深度缓解。在 26 例临床缓解的患者中,10 例 MRI 显示瘘管持续存在炎症(T2 高信号, = 7;对比增强, = 10)。单变量分析显示,深度缓解与直肠受累缺失以及抗 TNF-α 治疗转换或手术需求缺失相关。多变量分析表明,仅直肠受累缺失(OR = 4.6;95%CI:1.03-20.5)与深度缓解相关。
在接受维持抗 TNF-α 治疗的患者中,约有三分之一达到深度缓解。直肠受累缺失是深度缓解的预测因素。