Lee Jung-Hee, Park Jong-Seon
Division of Cardiology, Yeungnam University Medical Center, Yeungnam University College of Medicine, 3170, Hyeonchung-ro, Nam-gu, Daegu, Korea.
BMC Cardiovasc Disord. 2017 Jul 11;17(1):186. doi: 10.1186/s12872-017-0621-3.
An aberrant origin of the left coronary artery (LCA) from the right coronary cusp (RCC) is an extremely rare congenital anomaly. We here report on successful percutaneous coronary intervention (PCI) in a patient presenting with acute coronary syndrome and an aberrant origin of the LCA from the RCC.
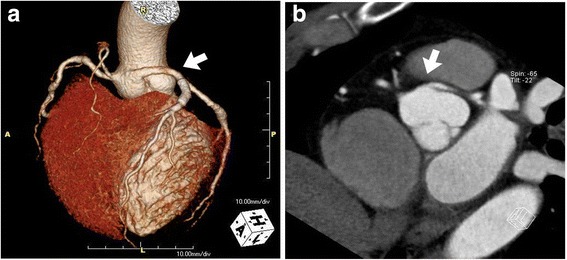
A 50-year-old man presented at our emergency department with recurrent resting chest pain. Following unsuccessful attempts at visualizing the left coronary artery using Judkins left and Amplatz catheters, an aortogram using a pigtail catheter suggested anomalous left coronary artery origin and showed a significant occlusive lesion at proximal left anterior descending artery. A Judkins right 4 guiding catheter was placed around the left coronary ostium and exchanged for a Judkins left 3.5 guiding catheter after introducing a .014" coronary long wire into the left circumflex artery. With excellent angiographic visualization and guide support, a drug-eluting stent was then successfully implanted. Cardiac computed tomography (CT) demonstrated left coronary artery origin from right coronary cusp.
This report presents a case of LCA originating from the RCC accompanied with acute coronary syndrome that was treated with successful PCI.
左冠状动脉(LCA)起源于右冠状动脉瓣叶(RCC)是一种极其罕见的先天性异常。我们在此报告一例患有急性冠状动脉综合征且左冠状动脉起源于右冠状动脉瓣叶的患者成功接受经皮冠状动脉介入治疗(PCI)的病例。
一名50岁男性因反复静息性胸痛就诊于我院急诊科。使用Judkins左导管和Amplatz导管未能成功显示左冠状动脉后,使用猪尾导管进行的主动脉造影提示左冠状动脉起源异常,并显示左前降支近端有明显的闭塞性病变。将Judkins右4导引导管置于左冠状动脉口周围,并在将一根0.014英寸冠状动脉长导丝引入左旋支动脉后,换成Judkins左3.5导引导管。在良好的血管造影显影和导引导管支撑下,随后成功植入一枚药物洗脱支架。心脏计算机断层扫描(CT)显示左冠状动脉起源于右冠状动脉瓣叶。
本报告介绍了一例左冠状动脉起源于右冠状动脉瓣叶并伴有急性冠状动脉综合征且成功接受PCI治疗的病例。