Vilela Leticia A P, Almeida Madson Q
Unidade de Suprarrenal, Endocrinologia do Desenvolvimento, Laboratório de Hormônios e Genética Molecular - LIM42, Divisão de Endocrinologia e Metabologia, Hospital das Clínicas, Faculdade de Medicina da Universidade de São Paulo (HCFMUSP), São Paulo, SP, Brasil.
Instituto do Câncer do Estado de São Paulo (Icesp), FMUSP, São Paulo, SP, Brasil.
Arch Endocrinol Metab. 2017 May-Jun;61(3):305-312. doi: 10.1590/2359-3997000000274.
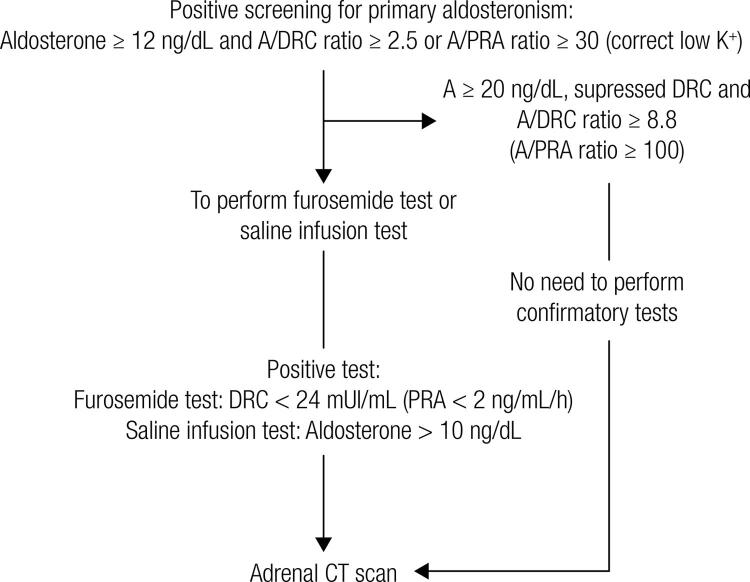
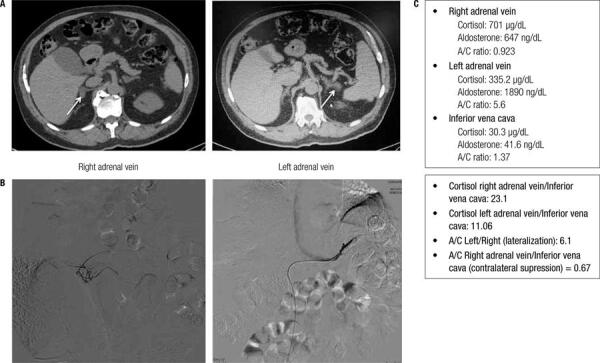
Primary aldosteronism (PA) is the most common form of secondary hypertension (HTN), with an estimated prevalence of 4% of hypertensive patients in primary care and around 10% of referred patients. Patients with PA have higher cardiovascular morbidity and mortality than age- and sex-matched patients with essential HTN and the same degree of blood pressure elevation. PA is characterized by an autonomous aldosterone production causing sodium retention, plasma renin supression, HTN, cardiovascular damage, and increased potassium excretion, leading to variable degrees of hypokalemia. Aldosterone-producing adenomas (APAs) account for around 40% and idiopathic hyperaldosteronism for around 60% of PA cases. The aldosterone-to-renin ratio is the most sensitive screening test for PA. There are several confirmatory tests and the current literature does not identify a "gold standard" confirmatory test for PA. In our institution, we recommend starting case confirmation with the furosemide test. After case confirmation, all patients with PA should undergo adrenal CT as the initial study in subtype testing to exclude adrenocortical carcinoma. Bilateral adrenal vein sampling (AVS) is the gold standard method to define the PA subtype, but it is not indicated in all cases. An experienced radiologist must perform AVS. Unilateral laparoscopic adrenalectomy is the preferential treatment for patients with APAs, and bilateral hyperplasia should be treated with mineralocorticoid antagonist (spironolactone or eplerenone). Cardiovascular morbidity caused by aldosterone excess can be decreased by either unilateral adrenalectomy or mineralocorticoid antagonist. In this review, we address the most relevant issues regarding PA screening, case confirmation, subtype classification, and treatment.
原发性醛固酮增多症(PA)是继发性高血压(HTN)最常见的形式,据估计,在初级保健的高血压患者中患病率为4%,在转诊患者中约为10%。与年龄和性别匹配、血压升高程度相同的原发性高血压患者相比,PA患者的心血管发病率和死亡率更高。PA的特征是醛固酮自主分泌,导致钠潴留、血浆肾素受抑制、高血压、心血管损害以及钾排泄增加,进而导致不同程度的低钾血症。醛固酮瘤(APA)约占PA病例的40%,特发性醛固酮增多症约占60%。醛固酮与肾素比值是PA最敏感的筛查试验。有几种确诊试验,目前的文献尚未确定PA的“金标准”确诊试验。在我们机构,我们建议从速尿试验开始进行病例确诊。病例确诊后,所有PA患者都应接受肾上腺CT检查,作为亚型检测的初始研究,以排除肾上腺皮质癌。双侧肾上腺静脉采血(AVS)是确定PA亚型的金标准方法,但并非适用于所有病例。必须由经验丰富的放射科医生进行AVS。单侧腹腔镜肾上腺切除术是APA患者的首选治疗方法,双侧增生应使用盐皮质激素拮抗剂(螺内酯或依普利酮)治疗。单侧肾上腺切除术或盐皮质激素拮抗剂均可降低醛固酮过多引起的心血管发病率。在本综述中,我们阐述了有关PA筛查、病例确诊、亚型分类和治疗的最相关问题。