Tilikete Caroline, Desestret Virginie
Neuro-Ophthalmology and Neurocognition, Hôpital Neurologique Pierre Wertheimer, Hospices Civils de Lyon, Bron, France.
Lyon I University, Lyon, France.
Front Neurol. 2017 Jun 29;8:302. doi: 10.3389/fneur.2017.00302. eCollection 2017.
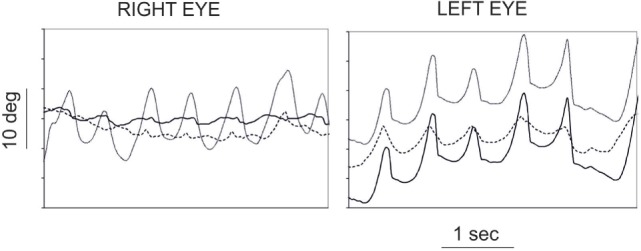
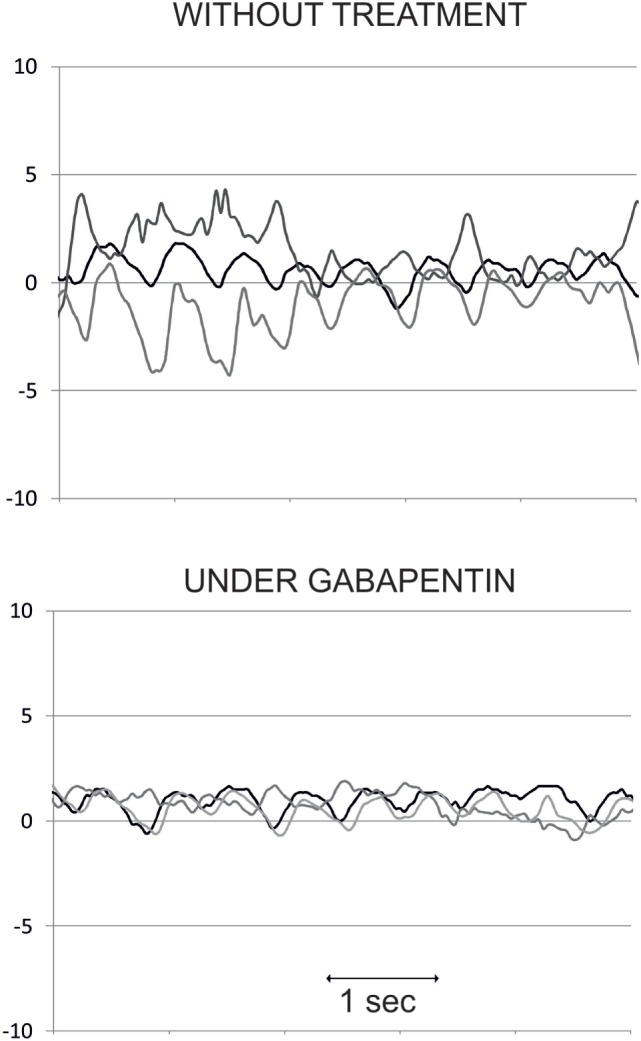
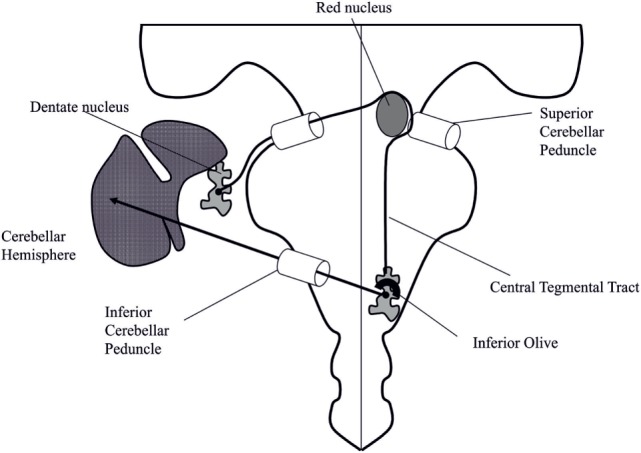
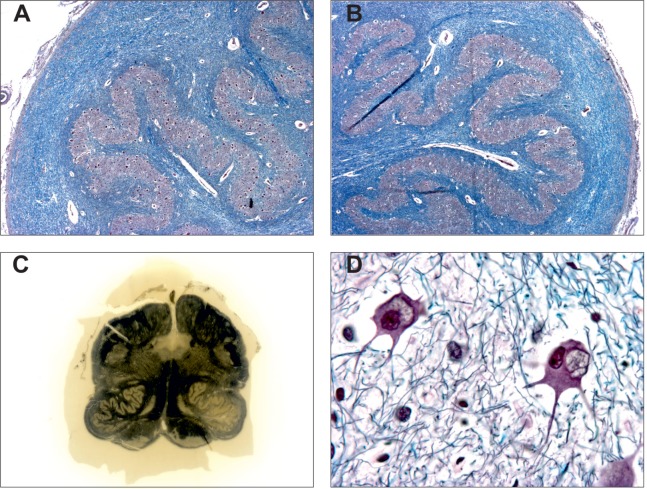
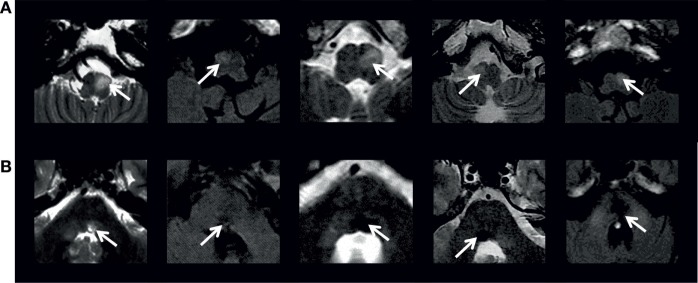
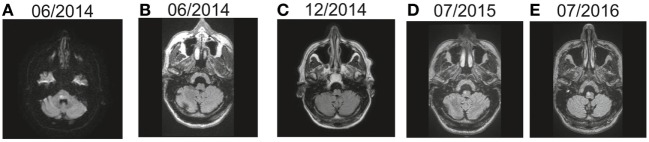
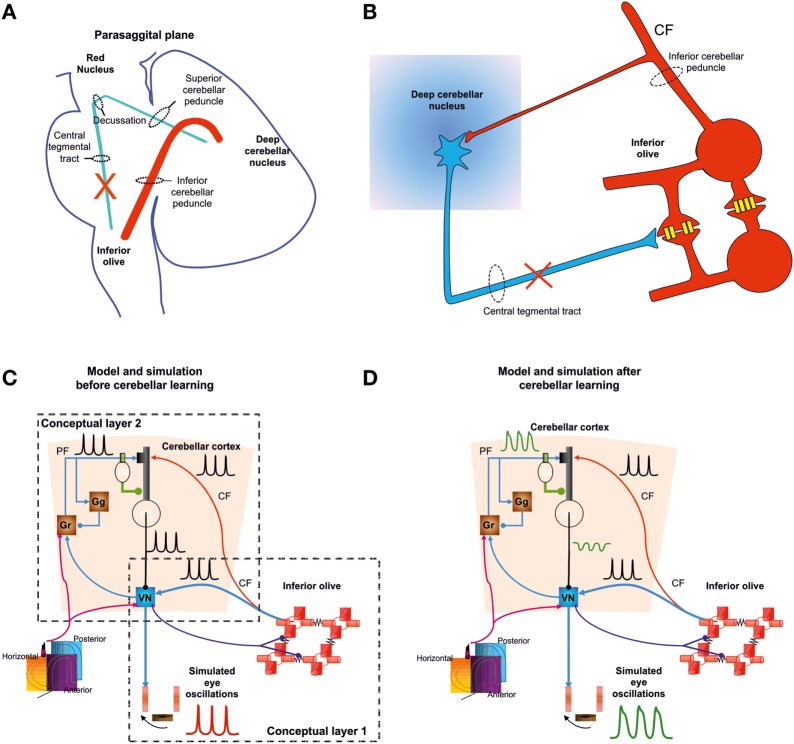
Hypertrophic degeneration of the inferior olive is mainly observed in patients developing palatal tremor (PT) or oculopalatal tremor (OPT). This syndrome manifests as a synchronous tremor of the palate (PT) and/or eyes (OPT) that may also involve other muscles from the branchial arches. It is associated with hypertrophic inferior olivary degeneration that is characterized by enlarged and vacuolated neurons, increased number and size of astrocytes, severe fibrillary gliosis, and demyelination. It appears on MRI as an increased T2/FLAIR signal intensity and enlargement of the inferior olive. There are two main conditions in which hypertrophic degeneration of the inferior olive occurs. The most frequent, studied, and reported condition is the development of PT/OPT and hypertrophic degeneration of the inferior olive in the weeks or months following a structural brainstem or cerebellar lesion. This "symptomatic" condition requires a destructive lesion in the Guillain-Mollaret pathway, which spans from the contralateral dentate nucleus the brachium conjunctivum and the ipsilateral central tegmental tract innervating the inferior olive. The most frequent etiologies of destructive lesion are stroke (hemorrhagic more often than ischemic), brain trauma, brainstem tumors, and surgical or gamma knife treatment of brainstem cavernoma. The most accepted explanation for this symptomatic PT/OPT is that denervated olivary neurons released from inhibitory inputs enlarge and develop sustained synchronized oscillations. The cerebellum then modulates/accentuates this signal resulting in abnormal motor output in the branchial arches. In a second condition, PT/OPT and progressive cerebellar ataxia occurs in patients without structural brainstem or cerebellar lesion, other than cerebellar atrophy. This syndrome of progressive ataxia and palatal tremor may be sporadic or familial. In the familial form, where hypertrophic degeneration of the inferior olive may not occur (or not reported), the main reported etiologies are Alexander disease, polymerase gamma mutation, and spinocerebellar ataxia type 20. Whether or not these are associated with specific degeneration of the dentato-olivary pathway remain to be determined. The most symptomatic consequence of OPT is eye oscillations. Therapeutic trials suggest gabapentin or memantine as valuable drugs to treat eye oscillations in OPT.
下橄榄核肥大性变性主要见于发生腭震颤(PT)或动眼-腭震颤(OPT)的患者。该综合征表现为腭部(PT)和/或眼部(OPT)的同步震颤,也可能累及鳃弓的其他肌肉。它与下橄榄核肥大性变性相关,其特征为神经元增大、空泡化,星形胶质细胞数量和大小增加,严重的纤维性胶质增生和脱髓鞘。在MRI上表现为下橄榄核T2/FLAIR信号强度增加和体积增大。下橄榄核肥大性变性主要发生在两种情况下。最常见、研究最多且报道最多的情况是在脑干或小脑结构性病变后的数周或数月内发生PT/OPT和下橄榄核肥大性变性。这种“症状性”情况需要在Guillain-Mollaret通路中有破坏性病变,该通路从对侧齿状核、结合臂延伸至支配下橄榄核的同侧中央被盖束。破坏性病变最常见的病因是中风(出血性比缺血性更常见)、脑外伤、脑干肿瘤以及脑干海绵状血管瘤的手术或伽玛刀治疗。对于这种症状性PT/OPT,最被认可的解释是,从抑制性输入中释放的失神经橄榄核神经元会增大并产生持续的同步振荡。然后小脑调节/增强该信号,导致鳃弓出现异常运动输出。在第二种情况下,除小脑萎缩外无脑干或小脑结构性病变的患者会出现PT/OPT和进行性小脑共济失调。这种进行性共济失调和腭震颤综合征可能是散发性的或家族性的。在家族性形式中,下橄榄核可能不发生肥大性变性(或未报道),主要报道的病因是亚历山大病、聚合酶γ突变和20型脊髓小脑共济失调。这些是否与齿状核-橄榄核通路的特定变性有关仍有待确定。OPT最明显的后果是眼球震颤。治疗试验表明加巴喷丁或美金刚是治疗OPT眼球震颤的有效药物。