Pankhurst Laura, Hudson Alex, Mumford Lisa, Willicombe Michelle, Galliford Jack, Shaw Olivia, Thuraisingham Raj, Puliatti Carmelo, Talbot David, Griffin Sian, Torpey Nicholas, Ball Simon, Clark Brendan, Briggs David, Fuggle Susan V, Higgins Robert M
NHS Blood and Transplant, Bristol, United Kingdom.
Renal and Transplant Unit, Hammersmith Hospital, London, United Kingdom.
Transplant Direct. 2017 Jun 26;3(7):e181. doi: 10.1097/TXD.0000000000000695. eCollection 2017 Jul.
ABO and HLA antibody incompatible (HLAi) renal transplants (AIT) now comprise around 10% of living donor kidney transplants. However, the relationship between pretransplant factors and medium-term outcomes are not fully understood, especially in relation to factors that may vary between centers.
The comprehensive national registry of AIT in the United Kingdom was investigated to describe the donor, recipient and transplant characteristics of AIT. Kaplan-Meier analysis was used to compare survival of AIT to all other compatible kidney transplants performed in the United Kingdom. Cox proportional hazards regression modeling was used to determine which pretransplant factors were associated with transplant survival in HLAi and ABOi separately. The primary outcome was transplant survival, taking account of death and graft failure.
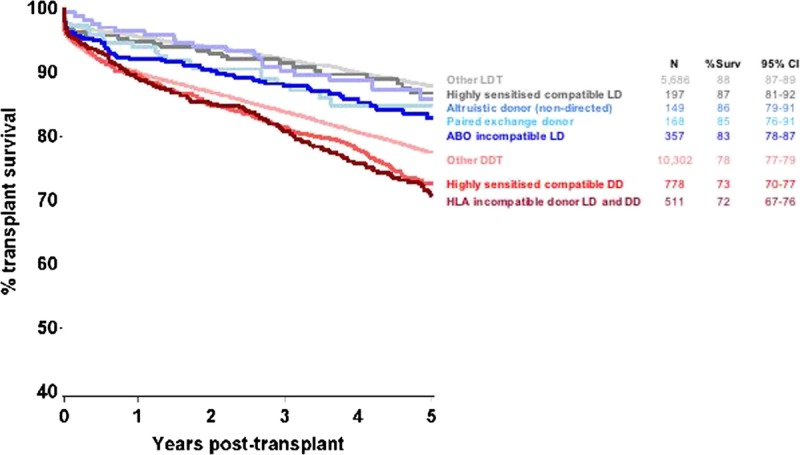
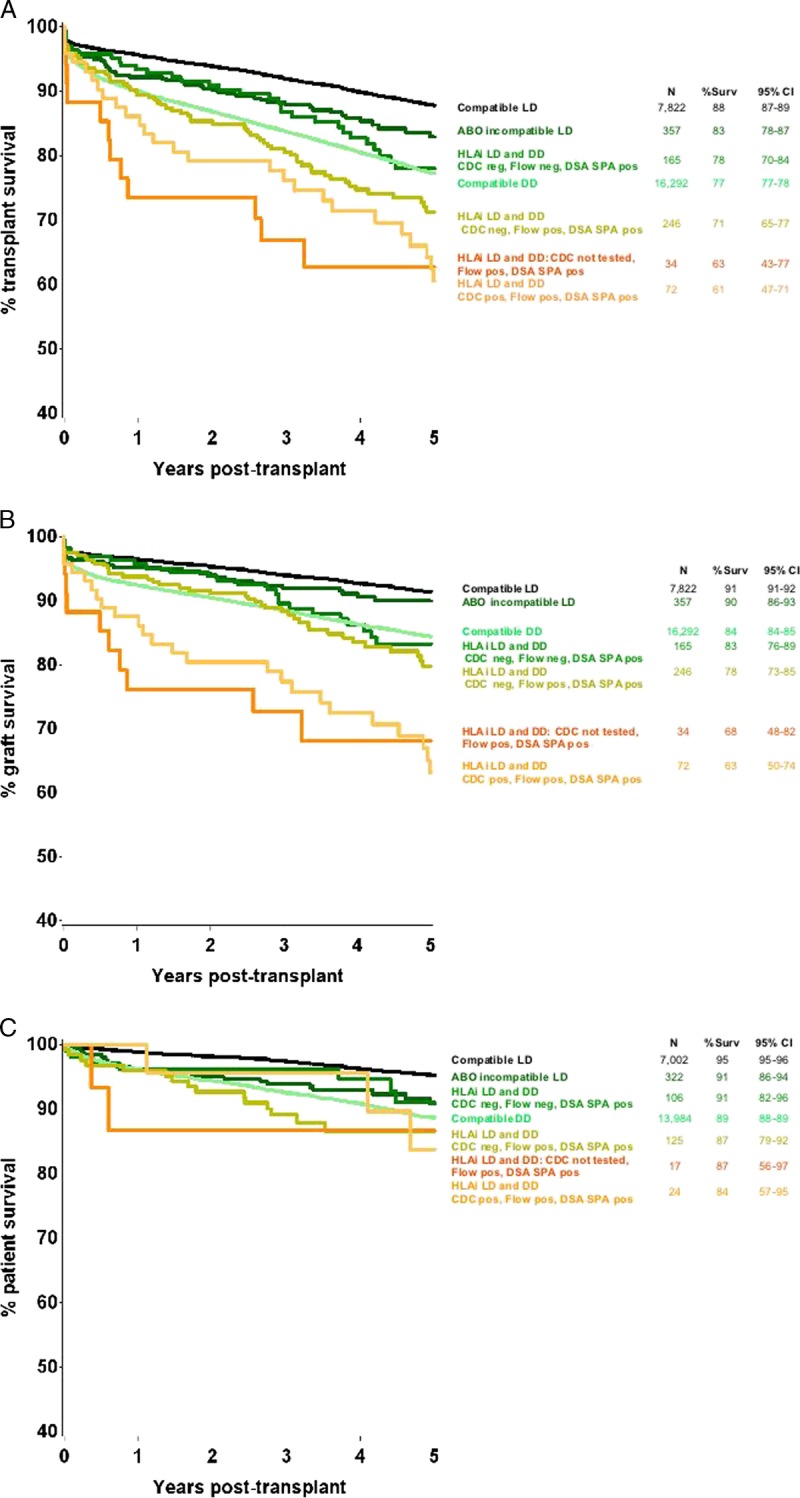
For 522 HLAi and 357 ABO incompatible (ABOi) transplants, 5-year transplant survival rates were 71% (95% confidence interval [CI], 66-75%) for HLAi and 83% (95% CI, 78-87%) for ABOi, compared with 88% (95% CI, 87-89%) for 7290 standard living donor transplants, and 78% (95% CI, 77-79%) for 15 322 standard deceased donor transplants ( < 0.0001). Increased chance of transplant loss in HLAi was associated with increasing number of donor specific HLA antibodies, center performing the transplant, antibody level at the time of transplant, and an interaction between donor age and dialysis status. In ABOi, transplant loss was associated with no use of IVIg, cytomegalovirus seronegative recipient, 000 HLA donor-recipient mismatch; and increasing recipient age.
Results of AIT were acceptable, certainly in the context of a choice between living donor AIT and an antibody compatible deceased donor transplant. Several factors were associated with increased chance of transplant loss, and these can lead to testable hypotheses for further improving therapy.
ABO血型和人类白细胞抗原抗体不相容(HLAi)的肾移植(AIT)目前约占活体供肾移植的10%。然而,移植前因素与中期结局之间的关系尚未完全明确,尤其是在不同中心可能存在差异的因素方面。
对英国AIT的全国综合登记系统进行调查,以描述AIT的供体、受体和移植特征。采用Kaplan-Meier分析比较AIT与英国进行的所有其他相容性肾移植的生存率。使用Cox比例风险回归模型分别确定哪些移植前因素与HLAi和ABOi中的移植存活相关。主要结局是考虑死亡和移植物失功的移植存活情况。
对于522例HLAi移植和357例ABO血型不相容(ABOi)移植,HLAi的5年移植生存率为71%(95%置信区间[CI],66 - 75%),ABOi为83%(95%CI,78 - 87%),相比之下,7290例标准活体供肾移植的5年移植生存率为88%(95%CI,87 - 89%),15322例标准尸体供肾移植为78%(95%CI,77 - 79%)(P < 0.0001)。HLAi中移植失败几率增加与供体特异性HLA抗体数量增加、进行移植的中心、移植时的抗体水平以及供体年龄与透析状态之间的相互作用有关。在ABOi中,移植失败与未使用静脉注射免疫球蛋白、巨细胞病毒血清学阴性受体、0/0 HLA供受体错配以及受体年龄增加有关。
AIT的结果是可以接受的,当然是在活体供体AIT和抗体相容的尸体供肾移植之间进行选择的情况下。几个因素与移植失败几率增加有关,并可据此提出可检验的假设以进一步改善治疗。