Nishimura Nao, Kasahara Mureo, Ishikura Kenji, Nakagawa Satoshi
Division of Critical Care Medicine, Department of Critical Care and Anesthesia, National Center for Child Health and Development, Ohkura 2-1-1, Setagaya, Tokyo, Japan.
Organ Transplantation Center, National Center for Child Health and Development, Ohkura 2-1-1, Setagaya, Tokyo, Japan.
J Intensive Care. 2017 Jul 20;5:48. doi: 10.1186/s40560-017-0241-0. eCollection 2017.
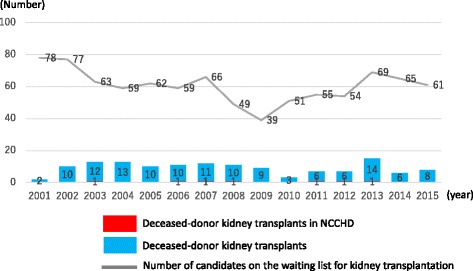
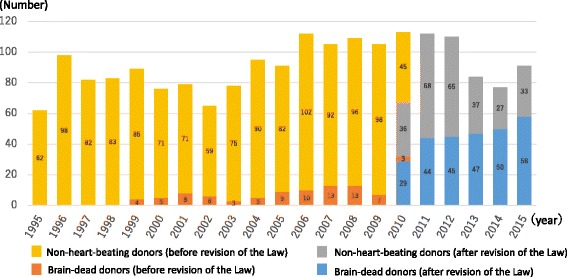
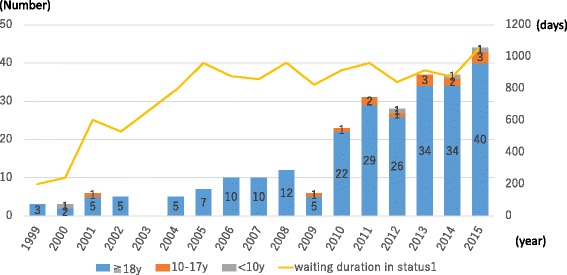
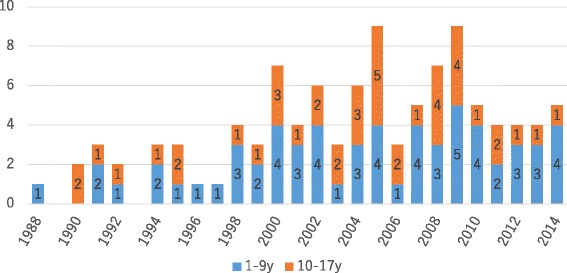
Brain-dead donor organ transplantation has been available to children in Japan since the 2010 revision of the Organ Transplant Law. Of the 50-60 brain-dead donor organ transplants performed annually in Japan, however, very few (0-4 per year) are performed in children. Again, while those receiving liver, heart, and kidney transplants are reported to fare better than their counterparts in the rest of the world, organ shortage is becoming a matter of great concern. Very few organs become available from brain-dead donors or are transplanted to adults if made available at all, with some children dying while on the brain-dead organ waiting list. Against this background, living-donor transplants, split-liver transplants, domino transplants, and hepatocyte transplants represent alternative modalities, each of which is shown to be associated with favorable outcomes. Challenges exist, include streamlining the existing framework for promoting organ donation for children and between children.
自2010年《器官移植法》修订以来,日本已开始为儿童进行脑死亡供体器官移植。然而,在日本每年进行的50至60例脑死亡供体器官移植中,儿童患者极少(每年0至4例)。此外,虽然据报道接受肝脏、心脏和肾脏移植的儿童比世界其他地区的同龄人情况更好,但器官短缺正成为一个令人极为担忧的问题。脑死亡供体提供的可用器官极少,即便有可用器官,也很少移植给成人,一些儿童在等待脑死亡器官移植的名单上死亡。在此背景下,活体供体移植、劈离式肝移植、多米诺移植和肝细胞移植成为替代方式,每种方式都显示出良好的效果。存在的挑战包括简化现有的促进儿童器官捐赠以及儿童之间器官捐赠的框架。