Toda Yuichiro, Sugimoto Kentaro
Department of Anesthesiology and Intensive Care Medicine, Kawasaki Medical School, 577 Matsushima, Kurashiki-shi, Okayama 701-0192 Japan.
Department of Anesthesiology and Resuscitology, Okayama University Medical School, Okayama, Japan.
J Intensive Care. 2017 Jul 20;5:49. doi: 10.1186/s40560-017-0242-z. eCollection 2017.
Acute kidney injury (AKI) after cardiac surgery in children with congenital heart disease is a common complication. AKI is also associated with high morbidity and mortality. The Kidney Diseases Improving Global Outcomes (KDIGO) criteria for AKI classification are now widely used for the definition of AKI. It is noteworthy that a statement about children was added to the criteria. Many studies aimed at finding useful biomarkers are now being performed by using these criteria. Clinicians should be aware of the recent progress in understanding AKI in children.
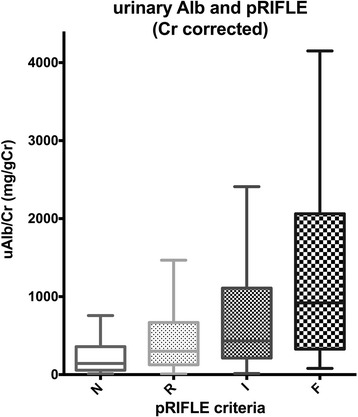
Unlike adult patients, young age is one of the major risk factors for AKI in pediatric cardiac surgery. The mechanism of the development of AKI in children might be different from that in adults because the surgical procedure and CPB technique in pediatric patients are greatly different from those in adult patients. There are many biomarkers for early detection of AKI, and some of them are widely used in hospitals. One of the major benefits of such biomarkers is the rapidness of expression for detecting increases in their expression levels. Neutrophil gelatinase-associated lipocalin, kidney injury molecule-1, cystatin C, and albumin have been investigated in some studies, and the usefulness of these biomarkers for detection of AKI and diagnosis of disease severity has been shown. Although there are many interventions for preventing and treating AKI after cardiac surgery in children, there is still no specific effective treatment. Peritoneal dialysis is effective for only maintaining a negative fluid balance early after cardiac surgery. The long-term prognosis of AKI is an issue of interest. Although mortality and morbidity of AKI in the acute phase of disease remain high, the long-term condition in pediatric patients is relatively acceptable unlike in adults.
KDIGO criteria are advocated as a diagnostic tool for common perception. Early recognition and intervention for AKI can be achieved by using several biomarkers. Further studies are needed to establish effective treatment for AKI.
先天性心脏病患儿心脏手术后发生急性肾损伤(AKI)是一种常见并发症。AKI还与高发病率和高死亡率相关。改善全球肾脏病预后组织(KDIGO)的AKI分类标准目前被广泛用于AKI的定义。值得注意的是,该标准中增加了关于儿童的说明。目前许多旨在寻找有用生物标志物的研究正在使用这些标准进行。临床医生应了解儿童AKI认识方面的最新进展。
与成年患者不同,低龄是小儿心脏手术中AKI的主要危险因素之一。儿童AKI的发生机制可能与成人不同,因为小儿患者的手术操作和体外循环技术与成人患者有很大差异。有许多用于早期检测AKI的生物标志物,其中一些在医院中广泛使用。此类生物标志物的主要优点之一是其表达迅速,可检测其表达水平的升高。中性粒细胞明胶酶相关脂质运载蛋白、肾损伤分子-1、胱抑素C和白蛋白已在一些研究中得到调查,这些生物标志物在检测AKI和诊断疾病严重程度方面的有用性已得到证实。虽然有许多干预措施用于预防和治疗儿童心脏手术后的AKI,但仍然没有特效治疗方法。腹膜透析仅在心脏手术后早期对维持负水平衡有效。AKI的长期预后是一个值得关注的问题。虽然疾病急性期AKI的死亡率和发病率仍然很高,但与成人不同,小儿患者的长期情况相对可以接受。
提倡将KDIGO标准作为一种普遍认可的诊断工具。使用几种生物标志物可实现对AKI的早期识别和干预。需要进一步研究以确立有效的AKI治疗方法。