Lakin Natasha, Rulach Robert, Nowicki Stefan, Kurian Kathreena M
Brain Tumour Research Group, Institute of Clinical Neurosciences, Level 1, Learning and Research Building, Southmead Hospital, University of Bristol, Bristol, United Kingdom.
The Beatson West of Scotland Cancer Centre, Glasgow, United Kingdom.
Front Oncol. 2017 Jul 6;7:141. doi: 10.3389/fonc.2017.00141. eCollection 2017.
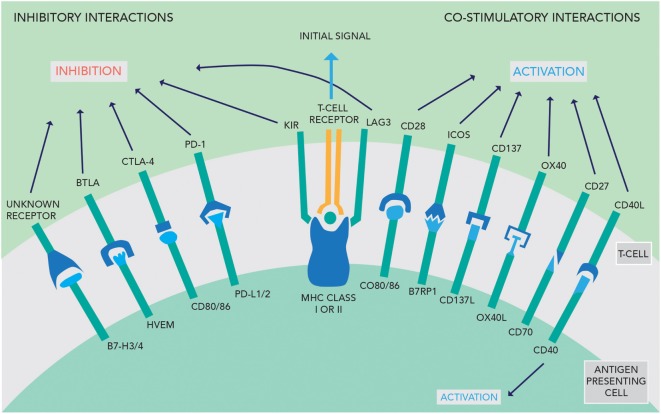
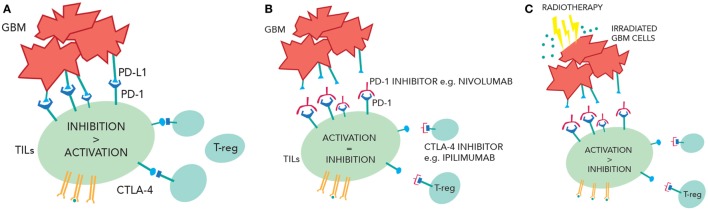
The adaptive immune system depends on the sequence of antigen presentation, activation, and then inhibition to mount a proportionate response to a threat. Tumors evade the immune response partly by suppressing T-cell activity using immune checkpoints. The use of cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), programmed cell death 1 (PD-1), and programmed cell death ligand 1 (PD-L1) antibodies counteract this suppression, thereby enhancing the antitumor activity of the immune system. This approach has proven efficacy in melanoma, renal cancer, and lung cancer. There is growing evidence that the central nervous system is accessible to the immune system in the diseased state. Moreover, glioblastomas (GBMs) attract CTLA-4-expressing T-cells and express PD-L1, which inhibit activation and continuation of a cytotoxic T-cell response, respectively. This may contribute to the evasion of the host immune response by GBM. Trials are in progress to determine if checkpoint inhibitors will be of benefit in GBM. Radiotherapy could also be helpful in promoting inflammation, enhancing the immunogenicity of tumors, disrupting the blood-brain barrier and creating greater antigen release. The combination of radiotherapy and checkpoint inhibitors has been promising in preclinical trials but is yet to show efficacy in humans. In this review, we summarize the mechanism and current evidence for checkpoint inhibitors in gliomas and other solid tumors, examine the rationale of combining radiotherapy with checkpoint inhibitors, and discuss the potential benefits and pitfalls of this approach.
适应性免疫系统依赖于抗原呈递、激活然后抑制的顺序,以对威胁做出适度反应。肿瘤部分通过使用免疫检查点抑制T细胞活性来逃避免疫反应。使用细胞毒性T淋巴细胞相关蛋白4(CTLA-4)、程序性细胞死亡蛋白1(PD-1)和程序性细胞死亡配体1(PD-L1)抗体可抵消这种抑制作用,从而增强免疫系统的抗肿瘤活性。这种方法已在黑色素瘤、肾癌和肺癌中证明有效。越来越多的证据表明,在患病状态下,免疫系统可进入中枢神经系统。此外,胶质母细胞瘤(GBM)吸引表达CTLA-4的T细胞并表达PD-L1,它们分别抑制细胞毒性T细胞反应的激活和持续。这可能有助于GBM逃避宿主免疫反应。正在进行试验以确定检查点抑制剂对GBM是否有益。放射治疗也可能有助于促进炎症、增强肿瘤的免疫原性、破坏血脑屏障并产生更多抗原释放。放射治疗和检查点抑制剂的联合在临床前试验中前景良好,但尚未在人体中显示出疗效。在本综述中,我们总结了胶质瘤和其他实体瘤中检查点抑制剂的机制和当前证据,研究了将放射治疗与检查点抑制剂联合使用的基本原理,并讨论了这种方法的潜在益处和风险。