Rasmussen Svein, Ebbing Cathrine, Irgens Lorentz M
Department of Clinical Science, University of Bergen, Bergen, Norway.
Department of Obstetrics and Gynaecology, Haukeland University Hospital, Bergen, Norway.
PLoS One. 2017 Jul 24;12(7):e0181016. doi: 10.1371/journal.pone.0181016. eCollection 2017.
To assess whether women with a history of preterm birth, independent on the presence of prelabour rupture of the membranes (PROM) and growth deviation of the newborn, are more likely to develop preeclampsia with preterm or preterm birth in a subsequent pregnancy.
We conducted a population-based cohort study, based on Medical Birth Registry of Norway between 1967 and 2012, including 742,980 women with singleton pregnancies who were followed up from their 1st to 2nd pregnancy. In the analyses we included 712,511 women after excluding 30,469 women with preeclampsia in the first pregnancy.
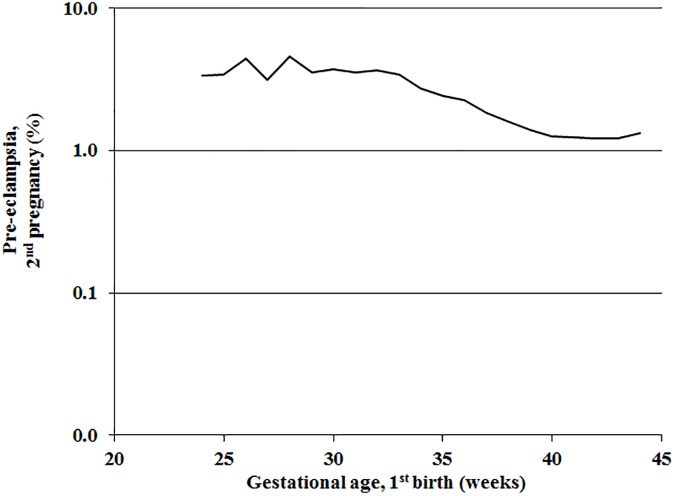
After preterm birth without preeclampsia in the first pregnancy, the risk of preterm preeclampsia in the second pregnancy was 4-7 fold higher than after term birth (odds ratios 3.5; 95% confidence interval (CI) 3.0-4.0 to 6.5; 95% CI 5.1-8.2). The risk of term preeclampsia in the pregnancy following a preterm birth was 2-3 times higher than after term birth (odds ratios 1.6; 95% CI 1.5-1.8 to 2.6; 95% CI 2.0-3.4). After spontaneous non-PROM preterm birth and preterm PROM, the risk of preterm preeclampsia was 3.3-3.6 fold higher than after spontaneous term birth. Corresponding risks of term preeclampsia was 1.6-1.8 fold higher. No significant time trends were found in the effect of spontaneous preterm birth in the first pregnancy on preterm or term preeclampsia in the second pregnancy.
The results suggest that preterm birth, regardless of the presence of PROM, and preeclampsia share pathophysiologic mechanisms. These mechanisms may cause preterm birth in one pregnancy and preeclampsia in a subsequent pregnancy in the same woman. The association was particularly evident with preterm preeclampsia.
评估有早产史的女性,无论是否存在胎膜早破(PROM)及新生儿生长发育异常,在随后的妊娠中发生早产或早产伴子痫前期的可能性是否更高。
我们基于挪威医疗出生登记处1967年至2012年的数据进行了一项基于人群的队列研究,纳入742,980名单胎妊娠女性,从首次妊娠至第二次妊娠进行随访。分析中排除了首次妊娠患有子痫前期的30,469名女性,纳入712,511名女性。
首次妊娠早产且无子痫前期者,第二次妊娠发生早产子痫前期的风险比足月分娩后高4至7倍(优势比3.5;95%置信区间(CI)3.0 - 4.0至6.5;95% CI 5.1 - 8.2)。早产后继发妊娠发生足月子痫前期的风险比足月分娩后高2至3倍(优势比1.6;95% CI 1.5 - 1.8至2.6;95% CI 2.0 - 3.4)。自然发生的非胎膜早破早产和早产伴胎膜早破后,发生早产子痫前期的风险比自然足月分娩后高3.3至3.6倍。足月子痫前期的相应风险高1.6至1.8倍。首次妊娠自然早产对第二次妊娠早产或足月子痫前期的影响未发现明显的时间趋势。
结果表明,早产,无论是否存在胎膜早破,与子痫前期具有共同的病理生理机制。这些机制可能导致同一女性一次妊娠发生早产,随后妊娠发生子痫前期。这种关联在早产子痫前期中尤为明显。