Delgado Anna F, Fahlström Markus, Nilsson Markus, Berntsson Shala G, Zetterling Maria, Libard Sylwia, Alafuzoff Irina, van Westen Danielle, Lätt Jimmy, Smits Anja, Larsson Elna-Marie
Department of Surgical Sciences, Radiology, Uppsala University, Uppsala, Sweden.
Department of Clinical Neuroscience, Karolinska Institute, Stockholm, Sweden.
Radiol Oncol. 2017 Feb 15;51(2):121-129. doi: 10.1515/raon-2017-0010. eCollection 2017 Jun.
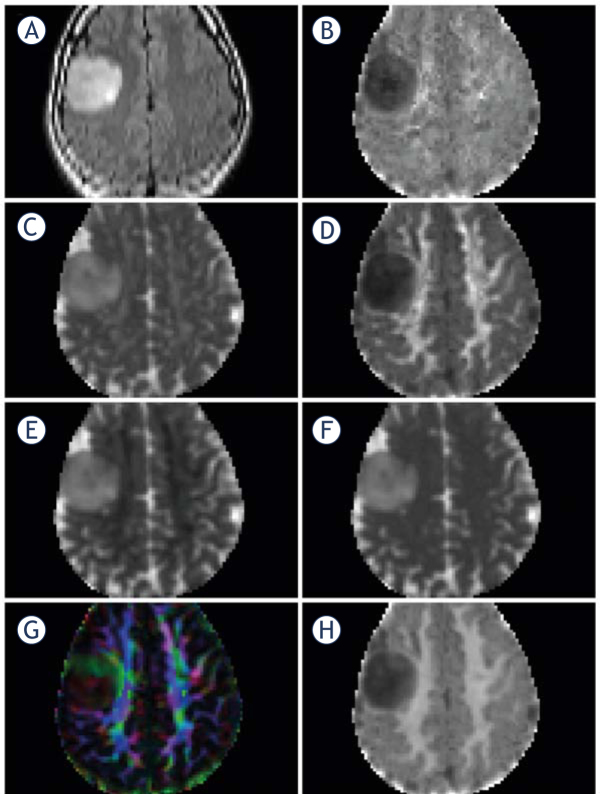
Diffusion kurtosis imaging (DKI) allows for assessment of diffusion influenced by microcellular structures. We analyzed DKI in suspected low-grade gliomas prior to histopathological diagnosis. The aim was to investigate if diffusion parameters in the perilesional normal-appearing white matter (NAWM) differed from contralesional white matter, and to investigate differences between glioma malignancy grades II and III and glioma subtypes (astrocytomas and oligodendrogliomas).
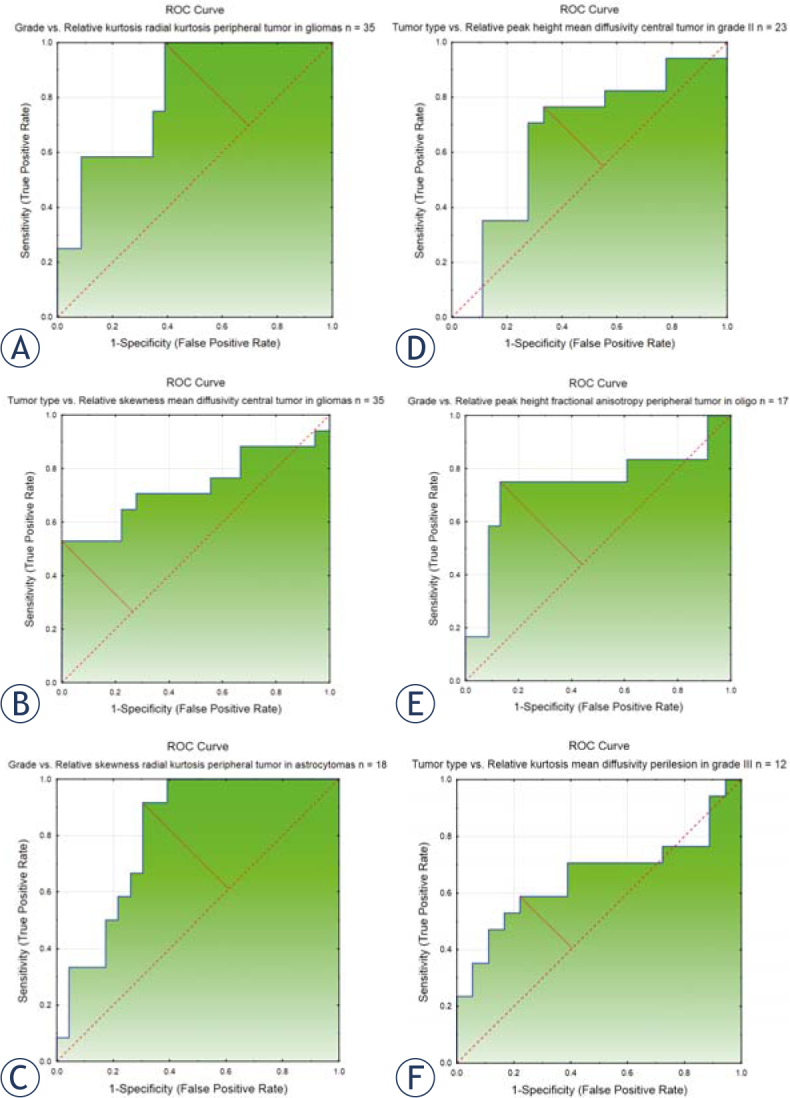
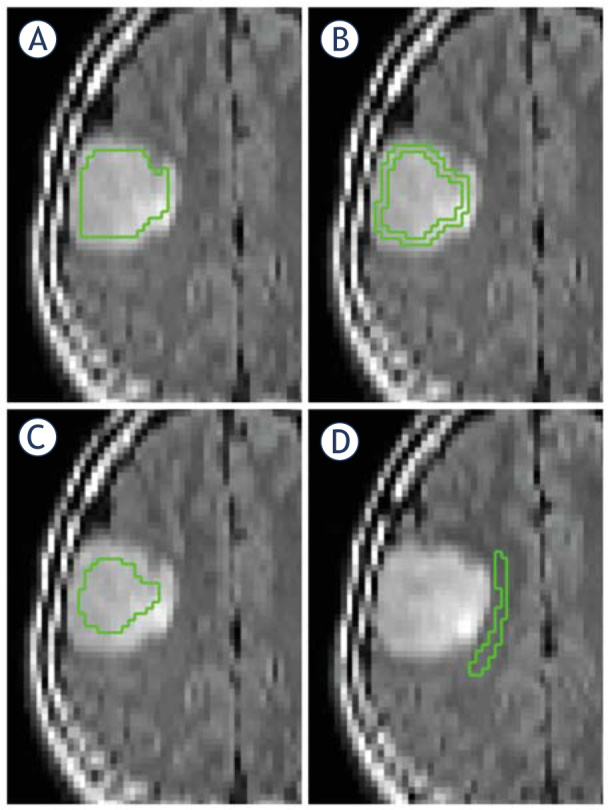
Forty-eight patients with suspected low-grade glioma were prospectively recruited to this institutional review board-approved study and investigated with preoperative DKI at 3T after written informed consent. Patients with histologically proven glioma grades II or III were further analyzed (n=35). Regions of interest (ROIs) were delineated on T2FLAIR images and co-registered to diffusion MRI parameter maps. Mean DKI data were compared between perilesional and contralesional NAWM (student's -test for dependent samples, Wilcoxon matched pairs test). Histogram DKI data were compared between glioma types and glioma grades (multiple comparisons of mean ranks for all groups). The discriminating potential for DKI in assessing glioma type and grade was assessed with receiver operating characteristics (ROC) curves.
There were significant differences in all mean DKI variables between perilesional and contralesional NAWM (=<0.000), except for axial kurtosis (=0.099). Forty-four histogram variables differed significantly between glioma grades II (n=23) and III (n=12) (p=0.003-0.048) and 10 variables differed significantly between ACs (n=18) and ODs (n=17) (=0.011-0.050). ROC curves of the best discriminating variables had an area under the curve (AUC) of 0.657-0.815.
Mean DKI variables in perilesional NAWM differ significantly from contralesional NAWM, suggesting altered microstructure by tumor infiltration not depicted on morphological MRI. Histogram analysis of DKI data identifies differences between glioma grades and subtypes.
扩散峰度成像(DKI)可用于评估受微细胞结构影响的扩散情况。我们在组织病理学诊断之前对疑似低级别胶质瘤进行了DKI分析。目的是研究瘤周正常外观白质(NAWM)中的扩散参数是否与对侧白质不同,以及研究胶质瘤II级和III级以及胶质瘤亚型(星形细胞瘤和少突胶质细胞瘤)之间的差异。
48例疑似低级别胶质瘤患者被前瞻性纳入本机构审查委员会批准的研究,并在签署书面知情同意书后于3T进行术前DKI检查。对组织学证实为II级或III级胶质瘤的患者进行进一步分析(n = 35)。在T2FLAIR图像上勾勒出感兴趣区域(ROI),并将其与扩散MRI参数图进行配准。比较瘤周和对侧NAWM之间的平均DKI数据(配对样本的学生t检验,Wilcoxon配对检验)。比较胶质瘤类型和胶质瘤级别之间的直方图DKI数据(所有组平均秩次的多重比较)。使用受试者工作特征(ROC)曲线评估DKI在评估胶质瘤类型和级别方面的鉴别潜力。
除轴向峰度(p = 0.099)外,瘤周和对侧NAWM之间所有平均DKI变量均存在显著差异(p <= 0.000)。44个直方图变量在胶质瘤II级(n = 23)和III级(n = 12)之间存在显著差异(p = 0.003 - 0.048),10个变量在星形细胞瘤(n = 18)和少突胶质细胞瘤(n = 17)之间存在显著差异(p = 0.011 - 0.050)。最佳鉴别变量的ROC曲线下面积(AUC)为0.657 - 0.815。
瘤周NAWM中的平均DKI变量与对侧NAWM有显著差异,提示肿瘤浸润导致微观结构改变,而形态学MRI未显示。DKI数据的直方图分析可识别胶质瘤级别和亚型之间的差异。