Sahu Biswanath, Abbey Pooja, Anand Rama, Kumar Ashok, Tomer Shaili, Malik Ekta
Department of Radio-Diagnosis, Lady Hardinge Medical College and Associated Hospitals, New Delhi, India.
Department of Surgery, Lady Hardinge Medical College and Associated Hospitals, New Delhi, India.
Indian J Radiol Imaging. 2017 Apr-Jun;27(2):152-160. doi: 10.4103/ijri.IJRI_300_16.
To assess the severity of acute pancreatitis (AP) using computed tomography (CT) severity index (CTSI) and modified CT severity index (MCTSI), to correlate with clinical outcome measures, and to assess concordance with severity grading, as per the revised Atlanta classification (RAC).
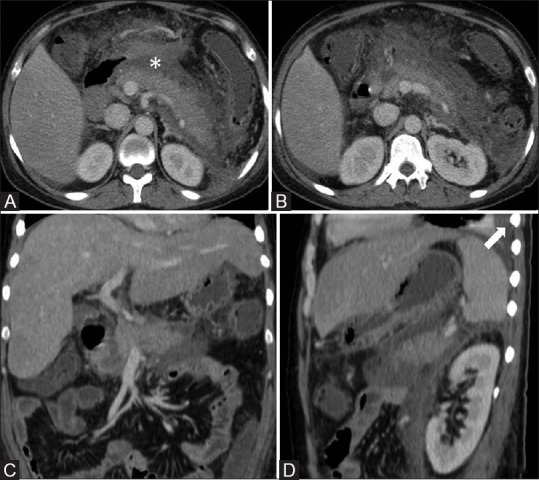
In this prospective study approved by the Institutional Review Board (November 2014 to March 2016), sixty patients with AP (as per the RAC definition) underwent contrast-enhanced computed tomography (CECT) 5-11 days (median 6 days) after symptom onset. Two radiologists, blinded to clinical parameters, independently assessed CTSI and MCTSI (differences were resolved by consensus). Clinical outcome parameters included duration of stay in the hospital and intensive care unit (ICU), presence of persistent organ failure (OF), evidence of infection, need for intervention, and mortality.
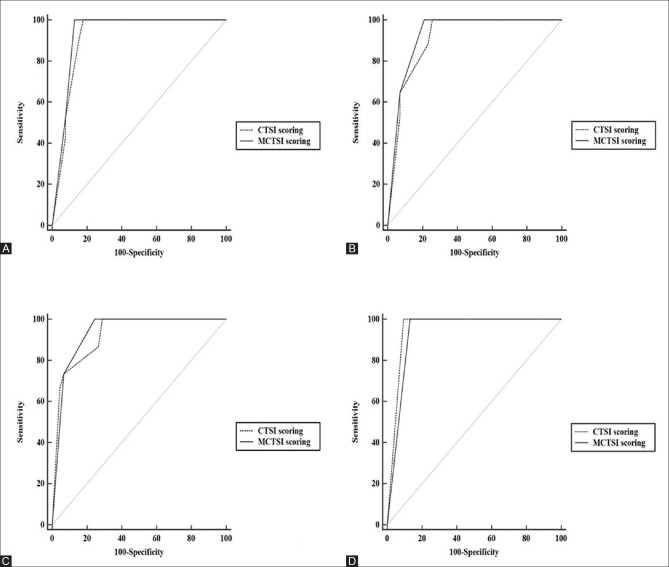
We included 60 cases [36 males, age range 19-65 (mean 37) years]. As per the RAC, 26 patients had mild AP, 12 moderately severe, and 22 severe AP. According to CTSI and MCTSI, mild, moderate, and severe cases were 27 (45%), 19 (31.7%), 14 (23.3%) and 24 (40%), 10 (16.7%), 26 (43.3%), respectively. MCTSI was concordant with the RAC grading in 54 (90.0%), CTSI was concordant in 47 (78.3%), and both were concordant in 43 (71.7%) cases. Area under the receiver-operating characteristic (ROC) curves (AUROC) was compared by the Hanley and McNeil method. Both CTSI and MCTSI were significantly associated with outcome parameters ( < 0.001), except duration of ICU stay. Sensitivity, specificity, positive predictive value (PPV), and accuracy of CTSI for detecting moderate/severe disease were 97.1%, 100%, 100%, and 98.3% respectively, and of MCTSI were 100%, 92.3%, 94.4%, and 96.7% respectively.
Both CTSI and MCTSI showed significant correlation with clinical outcome parameters, and good concordance with RAC grading of severity. MCTSI showed a higher sensitivity but lower specificity than CTSI in differentiating mild from moderate/severe AP.
使用计算机断层扫描(CT)严重程度指数(CTSI)和改良CT严重程度指数(MCTSI)评估急性胰腺炎(AP)的严重程度,将其与临床结局指标相关联,并根据修订的亚特兰大分类法(RAC)评估与严重程度分级的一致性。
在本项经机构审查委员会批准的前瞻性研究中(2014年11月至2016年3月),60例符合RAC定义的AP患者在症状发作后5 - 11天(中位时间6天)接受了增强计算机断层扫描(CECT)。两名对临床参数不知情的放射科医生独立评估CTSI和MCTSI(差异通过协商解决)。临床结局参数包括住院时间和重症监护病房(ICU)住院时间、持续性器官功能衰竭(OF)的存在、感染证据、干预需求和死亡率。
我们纳入了60例患者[36例男性,年龄范围19 - 65岁(平均37岁)]。根据RAC,26例患者为轻度AP,12例为中度重症,22例为重症AP。根据CTSI和MCTSI,轻度、中度和重度病例分别为27例(45%)、19例(31.7%)、14例(23.3%)和24例(40%)、10例(16.7%)、26例(43.3%)。MCTSI与RAC分级的一致性为54例(90.0%),CTSI为47例(78.3%),两者均一致的为43例(71.7%)。采用Hanley和McNeil方法比较受试者操作特征(ROC)曲线下面积(AUROC)。CTSI和MCTSI均与结局参数显著相关(<0.001),除了ICU住院时间。CTSI检测中度/重度疾病的敏感性、特异性、阳性预测值(PPV)和准确性分别为97.1%、100%、100%和98.3%,MCTSI分别为100%、92.3%、94.4%和96.7%。
CTSI和MCTSI均与临床结局参数显著相关,且与RAC严重程度分级具有良好的一致性。在区分轻度与中度/重度AP方面,MCTSI的敏感性高于CTSI,但特异性低于CTSI。