Department of Digestive and General Surgery, Faculty of Medicine, Shimane University, 89-1 Enya-cho, Izumo, Shimane, 693-8501, Japan.
World J Surg. 2018 Jan;42(1):172-184. doi: 10.1007/s00268-017-4144-y.
We describe a novel scoring system, namely the inflammatory response biomarker (IRB) score. The aim of this study is to evaluate the clinical value of IRB score in patients undergoing curative resection for esophageal squamous cell carcinoma (SCC).
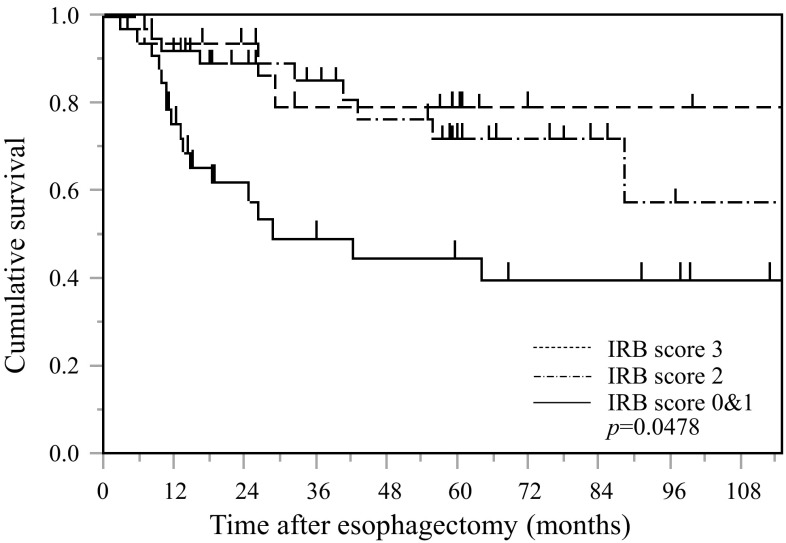
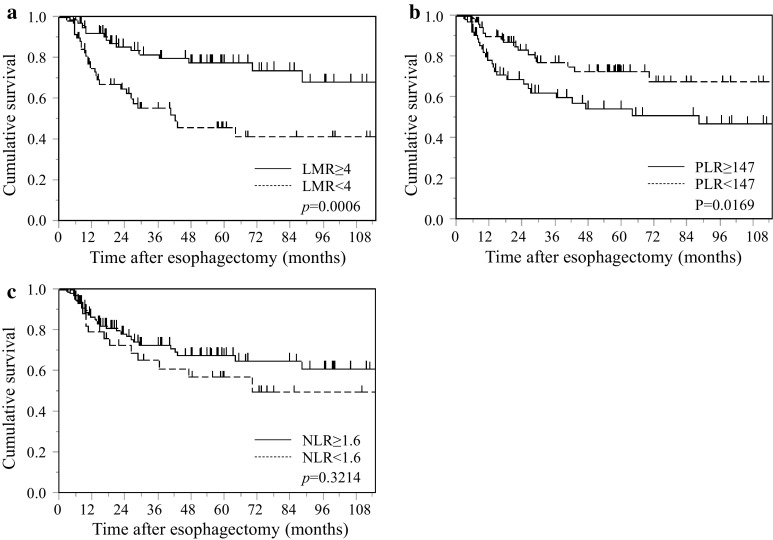
We retrospectively reviewed patients who underwent curative esophagectomy. We evaluated IRB score in both non-elderly (<70 years) and elderly (≥70 years) SCC patients. The IRB score was determined as follows: a high lymphocyte-to-monocyte ratio (LMR) (>4), a high neutrophil-to-lymphocyte ratio (NLR) (>1.6), and a low platelet-to-lymphocyte ratio (PLR) (<147) were each scored as 1, and the remaining values were scored as 0; the individual scores were then summed to produce the IRB score (range 0-3).
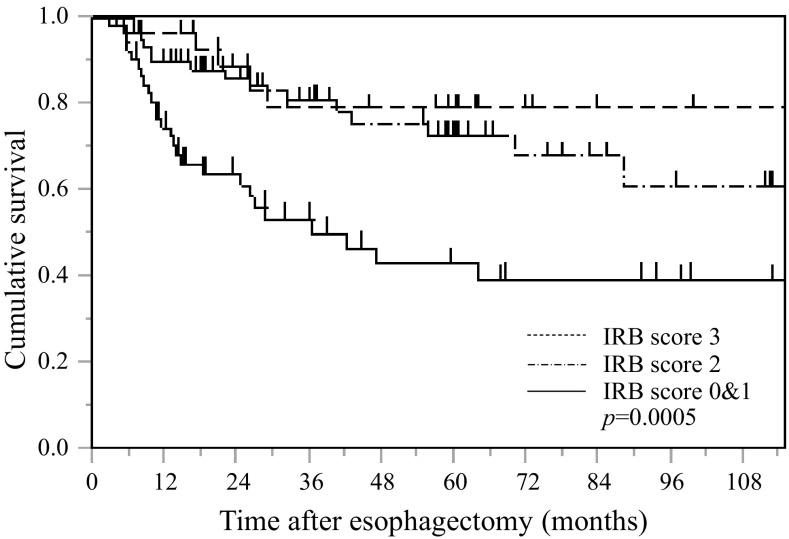
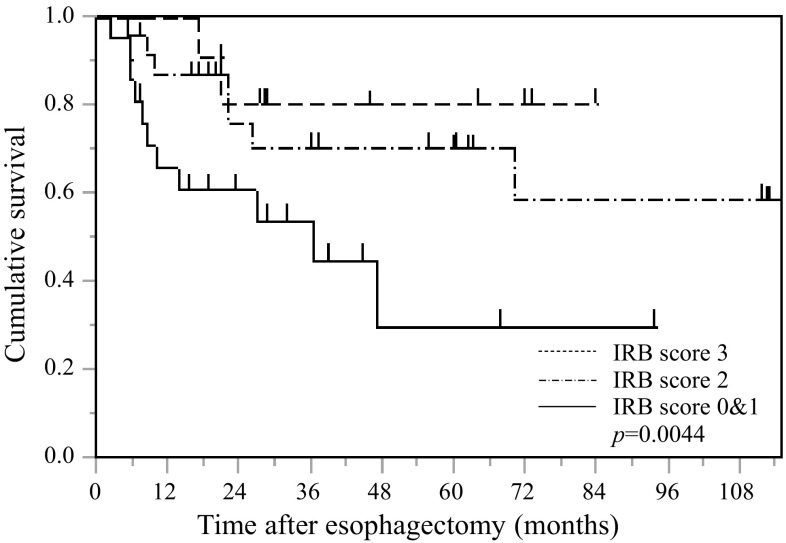
Univariate analyses demonstrated that the TNM pStage (p < 0.0001), tumor size (p = 0.002), LMR (p = 0.0057), PLR (p = 0.0328) and IRB score (p = 0.0003) were significant risk factors for a worse prognosis. On multivariate analysis, the TNM pStage (p < 0.0001) and IRB score (p = 0.0227) were independently associated with worse prognosis in overall patients. Among non-elderly patients, multivariate analyses demonstrated that the pStage (p = 0.0015) and IRB score (p = 0.0356) were independent risk factors for a worse prognosis. Among elderly patients, multivariate analysis demonstrated that the pStage (p = 0.0016), and IRB score (p = 0.0102) were independent risk factors for a worse prognosis.
The present study provides evidence that the preoperative IRB score can be considered a promising independent prognostic factor of cancer-specific survival in patients undergoing curative resection for SCC, and that its predictive ability is useful in both non-elderly and elderly patients.
我们描述了一种新的评分系统,即炎症反应生物标志物(IRB)评分。本研究旨在评估 IRB 评分在接受根治性食管鳞癌(SCC)切除术的患者中的临床价值。
我们回顾性分析了接受根治性食管切除术的患者。我们评估了非老年(<70 岁)和老年(≥70 岁)SCC 患者的 IRB 评分。IRB 评分如下确定:高淋巴细胞与单核细胞比值(LMR)(>4)、高中性粒细胞与淋巴细胞比值(NLR)(>1.6)和低血小板与淋巴细胞比值(PLR)(<147)各计 1 分,其余值计 0 分;然后将各分值相加得出 IRB 评分(范围 0-3)。
单因素分析表明,TNM p 分期(p<0.0001)、肿瘤大小(p=0.002)、LMR(p=0.0057)、PLR(p=0.0328)和 IRB 评分(p=0.0003)是预后较差的显著危险因素。多因素分析显示,TNM p 分期(p<0.0001)和 IRB 评分(p=0.0227)与总体患者的预后不良独立相关。在非老年患者中,多因素分析表明 p 分期(p=0.0015)和 IRB 评分(p=0.0356)是预后不良的独立危险因素。在老年患者中,多因素分析表明 p 分期(p=0.0016)和 IRB 评分(p=0.0102)是预后不良的独立危险因素。
本研究提供的证据表明,术前 IRB 评分可被视为 SCC 根治性切除术患者癌症特异性生存的有前途的独立预后因素,其预测能力在非老年和老年患者中均有用。