Setty Bhuvana A, Stanek Joseph R, Mascarenhas Leo, Miller Alexandra, Bagatell Rochelle, Okcu Fatih, Nicholls Lauren, Lysecki David, Gupta Abha A
Division of Hematology/Oncology/BMT, Nationwide Children's Hospital, Columbus, Ohio.
Division of Hematology, Oncology and Blood and Marrow Transplantation, Department of Pediatrics, Children's Hospital Los Angeles, Los Angeles, California.
Pediatr Blood Cancer. 2018 Jan;65(1). doi: 10.1002/pbc.26728. Epub 2017 Jul 27.
The combination of vincristine, irinotecan, and temozolomide (VIT) is often used to treat children and adolescents with relapsed rhabdomyosarcoma (RMS); however, the outcome of these patients has not been previously described.
We sought to determine the response rate (RR) and progression-free survival (PFS) for patients with relapsed RMS treated with VIT by retrospective review of patients treated at five tertiary care hospitals. Prior treatment with irinotecan was permitted.
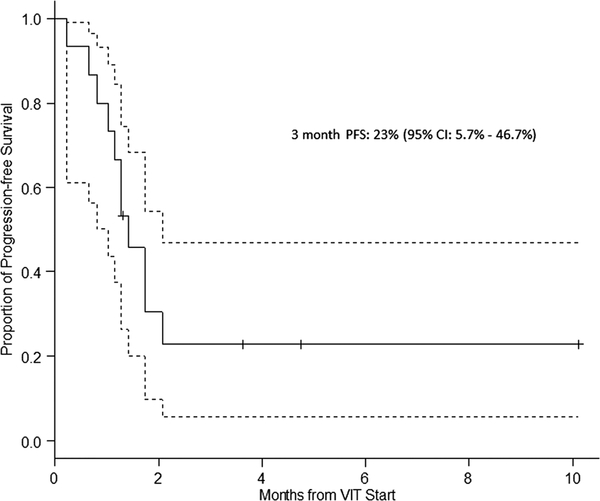
Among 19 patients with a median age of 8 years (range 2-17 years), 12 (63%) were males and 12 (63%) had embryonal histology. Median time to relapse from initial diagnosis was 16 months (range 2.8-45 months). VIT was used as first, second, third, or fourth line of therapy in four (21%), seven (37%), six (32%), and two (10%) patients, respectively. Four patients received VIT as adjuvant therapy following radiation and/or surgery. Therefore, among 15 evaluable patients, the best response to VIT was 0 (complete response, CR), 0 (partial response, PR), 4 (stable disease, SD), and 11 (progressive disease, PD) for an overall clinical benefit rate (CR + PR + SD) of 26.7% (95% CI: 7.8-55.1%). After a median follow-up of 8 months, 2 (10%) patients were alive without disease, 3 (16%) were alive with disease, and 14 (74%) patients died of PD. PFS at 3 months was 23% (95% CI: 5.7-46.7%).
VIT therapy in combination with adequate local control is associated with some disease control in patients with first relapse RMS and may be another reasonable option to offer patients as salvage therapy.
长春新碱、伊立替康和替莫唑胺(VIT)联合方案常用于治疗复发横纹肌肉瘤(RMS)的儿童和青少年;然而,此前尚未描述过这些患者的治疗结果。
我们通过回顾性分析五家三级医疗中心治疗的患者,试图确定接受VIT治疗的复发RMS患者的缓解率(RR)和无进展生存期(PFS)。允许患者之前接受过伊立替康治疗。
19例患者的中位年龄为8岁(范围2 - 17岁),其中12例(63%)为男性,12例(63%)为胚胎型组织学类型。从初始诊断到复发的中位时间为16个月(范围2.8 - 45个月)。VIT分别作为4例(21%)、7例(37%)、6例(32%)和2例(10%)患者的一线、二线、三线或四线治疗方案。4例患者在放疗和/或手术后接受VIT作为辅助治疗。因此,在15例可评估患者中,VIT的最佳反应为0例(完全缓解,CR)、0例(部分缓解,PR)、4例(疾病稳定,SD)和11例(疾病进展,PD),总体临床获益率(CR + PR + SD)为26.7%(95%CI:7.8 - 55.1%)。中位随访8个月后,2例(10%)患者无病存活,3例(16%)患者带病存活,14例(74%)患者死于疾病进展。3个月时的PFS为23%(95%CI:5.7 - 46.7%)。
VIT治疗联合充分的局部控制与首次复发RMS患者的部分疾病控制相关,可能是为患者提供挽救治疗的另一个合理选择。