Doukhan Laure, Bisbal Magali, Chow-Chine Laurent, Sannini Antoine, Brun Jean Paul, Cambon Sylvie, Nguyen Duong Lam, Faucher Marion, Mokart Djamel
Intensive Care Unit, Institut Paoli Calmettes, Marseille, France.
PLoS One. 2017 Jul 27;12(7):e0181808. doi: 10.1371/journal.pone.0181808. eCollection 2017.
Prognostic impact of delayed intensive care unit(ICU) admission in critically ill cancer patients remains debatable. We determined predictive factors for later ICU admission and mortality in cancer patients initially not admitted after their first ICU request.
All cancer patients referred for an emergency ICU admission between 1 January 2012 and 31 August 2013 were included.
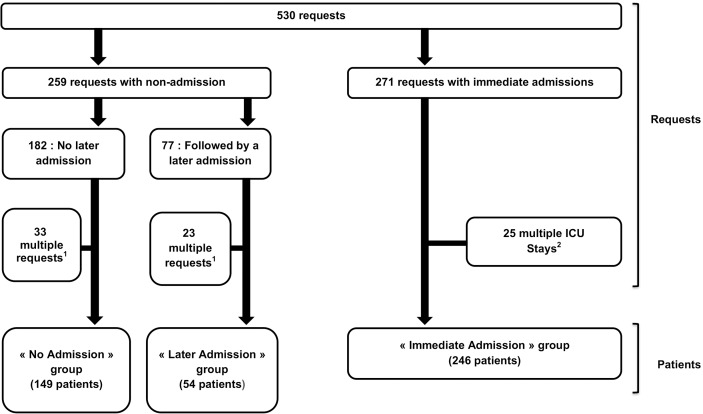
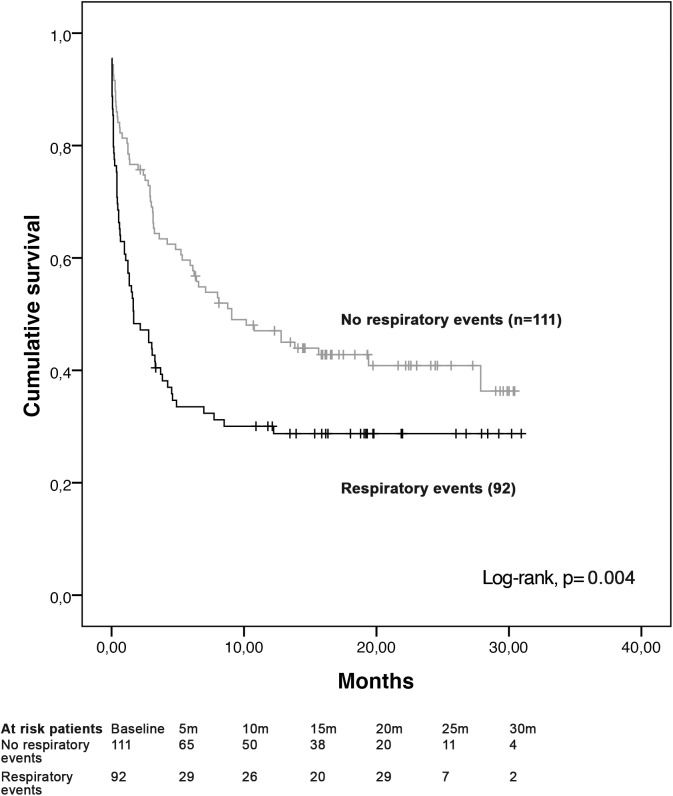
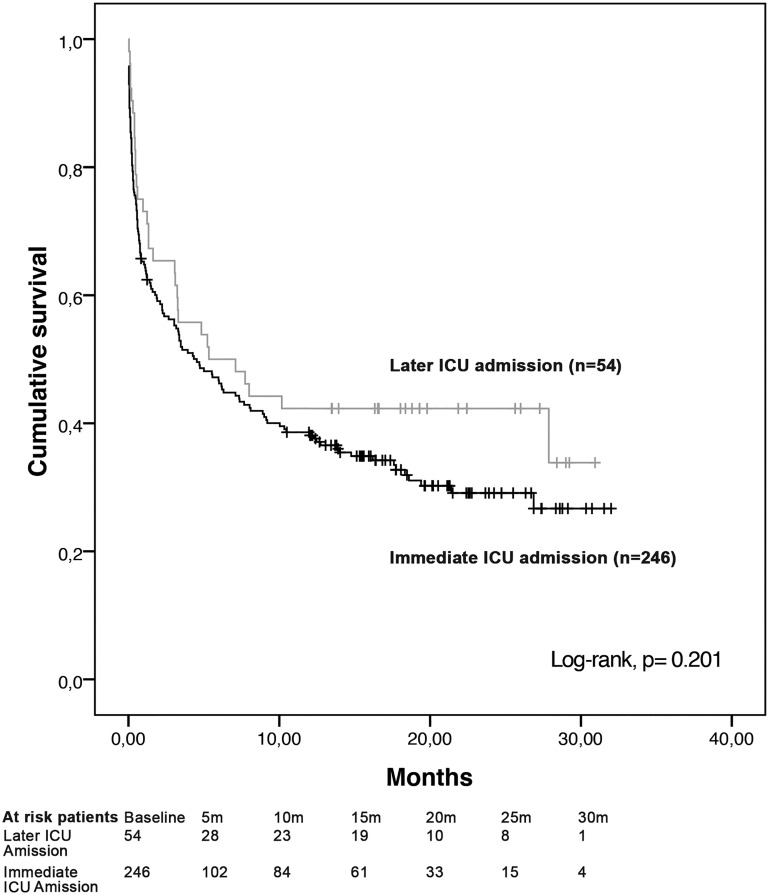
Totally, 246(54.8%) patients were immediately admitted. Among 203(45.2%) patients denied at the first request, 54(26.6%) were admitted later. A former ICU stay [OR: 2.75(1.12-6.75)], a request based on a clinical respiratory event[OR: 2.6(1.35-5.02)] and neutropenia[OR: 2.25(1.06-4.8)] were independently associated with later ICU admission. Survival of patients admitted immediately and later did not differ at ICU(78.5% and 70.4%, respectively; p = 0.2) or hospital(74% and 66%, respectively; p = 0.24) discharge. Hospital mortality of patients initially not admitted was 29.7% and independently associated with malignancy progression[OR: 3.15(1.6-6.19)], allogeneic hematopoietic stem cell transplantation[OR: 2.5(1.06-5.89)], a request based on a clinical respiratory event[OR: 2.36(1.22-4.56)] and severe sepsis[OR: 0.27(0.08-0.99)].
Compared with immediate ICU admission, later ICU admission was not associated with hospital mortality. Clinical respiratory events were independently associated with both later ICU admission and hospital mortality.
危重症癌症患者延迟入住重症监护病房(ICU)对预后的影响仍存在争议。我们确定了最初在首次提出ICU需求后未入住的癌症患者延迟入住ICU及死亡的预测因素。
纳入2012年1月1日至2013年8月31日期间因紧急情况转诊至ICU的所有癌症患者。
共有246例(54.8%)患者立即入住。在首次被拒绝的203例(45.2%)患者中,54例(26.6%)随后入住。既往曾入住ICU[比值比(OR):2.75(1.12 - 6.75)]、基于临床呼吸事件提出的需求[OR:2.6(1.35 - 5.02)]和中性粒细胞减少[OR:2.25(1.06 - 4.8)]与延迟入住ICU独立相关。立即入住和延迟入住患者在ICU出院时的生存率无差异(分别为78.5%和70.4%;p = 0.2),在医院出院时也无差异(分别为74%和66%;p = 0.24)。最初未入住患者的医院死亡率为29.7%,且与恶性肿瘤进展[OR:3.15(1.6 - 6.19)]、异基因造血干细胞移植[OR:2.5(1.06 - 5.89)]、基于临床呼吸事件提出的需求[OR:2.36(1.22 - 4.56)]和严重脓毒症[OR:0.27(0.08 - 0.99)]独立相关。
与立即入住ICU相比,延迟入住ICU与医院死亡率无关。临床呼吸事件与延迟入住ICU和医院死亡率均独立相关。