Hardie Diana Ruth, Korsman Stephen N, Hsiao Nei-Yuan, Morobadi Molefi Daniel, Vawda Sabeehah, Goedhals Dominique
Division of Virology, Department of Pathology, University of Cape Town, Cape Town, South Africa.
National Health Laboratory Service, South Africa.
PLoS One. 2017 Jul 31;12(7):e0182167. doi: 10.1371/journal.pone.0182167. eCollection 2017.
In South Africa where the prevalence of HIV infection is very high, 4th generation HIV antibody/p24 antigen combo immunoassays are the tests of choice for laboratory based screening. Testing is usually performed in clinical pathology laboratories on automated analysers. To investigate the cause of false positive results on 4th generation HIV testing platforms in public sector laboratories, the performance of two automated platforms was compared in a clinical pathology setting, firstly on routine diagnostic specimens and secondly on known sero-negative samples.
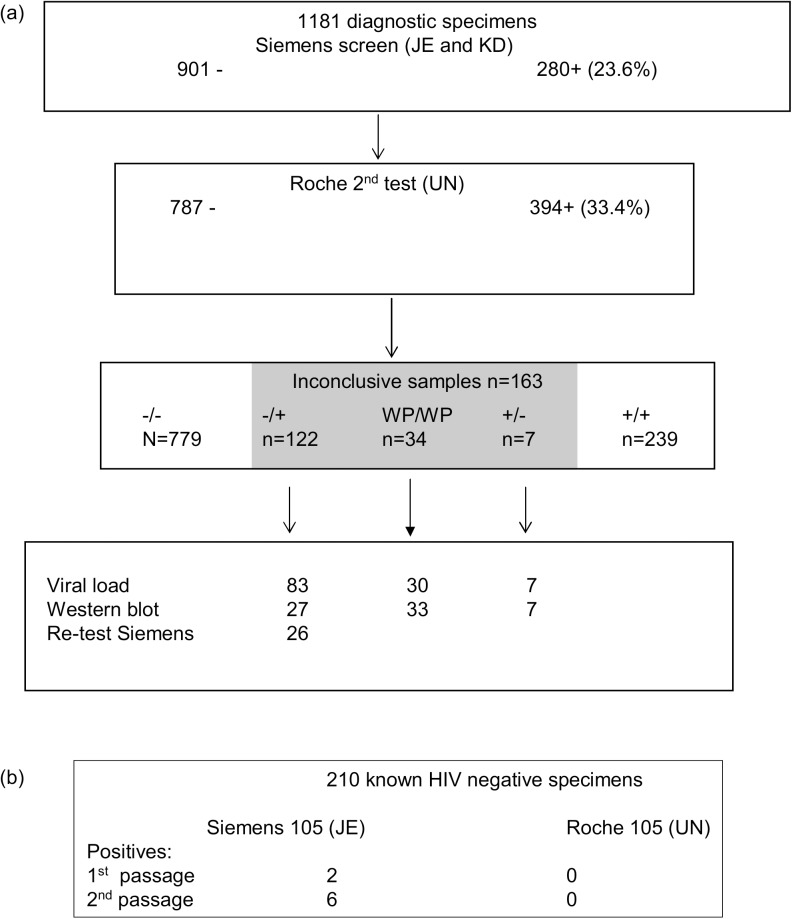
Firstly, 1181 routine diagnostic specimens were sequentially tested on Siemens and Roche automated 4th generation platforms. HIV viral load, western blot and follow up testing were used to determine the true status of inconclusive specimens. Subsequently, known HIV seronegative samples from a single donor were repeatedly tested on both platforms and an analyser was tested for surface contamination with HIV positive serum to identify how suspected specimen contamination could be occurring.
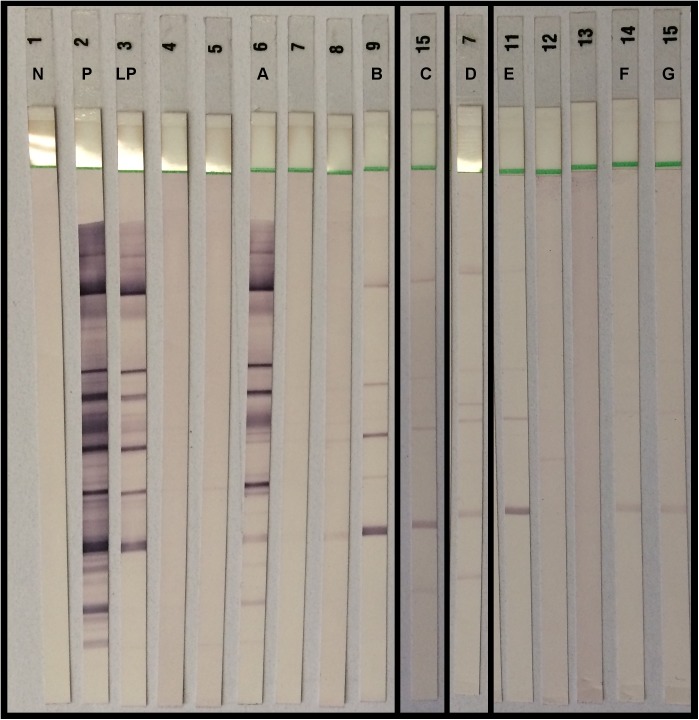
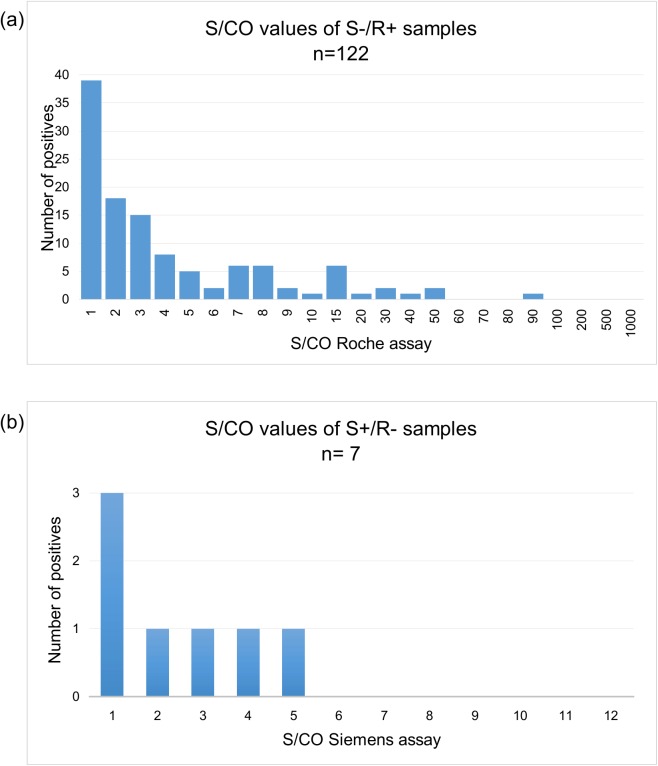
Serial testing of diagnostic specimens yielded 163 weakly positive or discordant results. Only 3 of 163 were conclusively shown to indicate true HIV infection. Specimen contamination with HIV antibody was suspected, based on the following evidence: the proportion of positive specimens increased on repeated passage through the analysers; viral loads were low or undetectable and western blots negative or indeterminate on problem specimens; screen negative, 2nd test positive specimens tested positive when reanalysed on the screening assay; follow up specimens (where available) were negative. Similarly, an increasing number of known negative specimens became (repeatedly) sero-positive on serial passage through one of the analysers. Internal and external analyser surfaces were contaminated with HIV serum, evidence that sample splashes occur during testing.
Due to the extreme sensitivity of these assays, contamination with minute amounts of HIV antibody can cause a negative sample to test positive. Better contamination control measures are needed on analysers used in clinical pathology environments, especially in regions where HIV sero-prevalence is high.
在南非,HIV感染率非常高,第四代HIV抗体/p24抗原联合免疫测定法是基于实验室筛查的首选检测方法。检测通常在临床病理实验室的自动分析仪上进行。为了调查公共部门实验室中第四代HIV检测平台出现假阳性结果的原因,在临床病理环境中比较了两个自动平台的性能,首先是对常规诊断标本进行检测,其次是对已知血清学阴性的样本进行检测。
首先,在西门子和罗氏自动第四代平台上对1181份常规诊断标本进行连续检测。使用HIV病毒载量、免疫印迹法和后续检测来确定不确定标本的真实状况。随后,对来自单一供体的已知HIV血清阴性样本在两个平台上进行重复检测,并对分析仪进行HIV阳性血清表面污染检测,以确定可能发生疑似标本污染的方式。
对诊断标本的连续检测产生了163个弱阳性或不一致的结果。163个结果中只有3个最终被证明表明存在真正的HIV感染。基于以下证据怀疑标本被HIV抗体污染:阳性标本在分析仪上重复检测时比例增加;问题标本的病毒载量低或无法检测到,免疫印迹法结果为阴性或不确定;筛查阴性、第二次检测阳性的标本在筛查试验中重新分析时呈阳性;后续标本(如有)为阴性。同样,越来越多已知的阴性标本在通过其中一台分析仪连续检测时(反复)变为血清阳性。分析仪的内部和外部表面被HIV血清污染,证明检测过程中会发生样本飞溅。
由于这些检测方法极其灵敏,微量HIV抗体污染可导致阴性样本检测呈阳性。临床病理环境中使用的分析仪需要更好的污染控制措施,尤其是在HIV血清流行率高的地区。