Division of Molecular and Clinical Cancer Sciences, Faculty of Biology, Medicine and Health, University of Manchester, St Mary’s Hospital, Manchester, England
Division of Evolution and Genomic Sciences, University of Manchester, St Mary’s Hospital, Manchester, England
JAMA Oncol. 2017 Dec 1;3(12):1702-1706. doi: 10.1001/jamaoncol.2017.0619.
Lynch syndrome is caused by dominantly inherited germline mutations that predispose individuals to colorectal, endometrial, ovarian, and other cancers through inactivation of the cellular mismatch repair system. Lynch syndrome–associated cancers are amenable to surveillance strategies that may improve survival. The age at which surveillance should start is disputed.
To determine whether mutated gene and type of mutation influence age at onset of Lynch syndrome–associated cancers.
DESIGN, SETTING, AND PARTICIPANTS: A retrospective cohort study of individuals with Lynch syndrome–associated colorectal, endometrial, and/or ovarian cancers whose medical records were included in the clinical database of a large quaternary referral center for genomic medicine in the Northwest of England.
Mutated gene (MLH1, MSH2, MSH6, and/or PMS2) and type of mutation (truncating, splicing, or large rearrangement).
Age at cancer diagnosis.
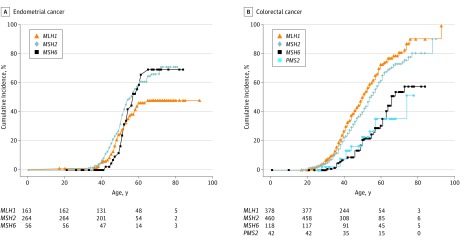
A total of 1063 individuals with proven Lynch syndrome were included, 495 male and 568 female (mean age 52 years; age range, 10-93 years [children were included in the database, but no children developed cancer]). There were 546 men and women with colorectal cancer, 162 women with endometrial cancer, and 49 women with ovarian cancer; mean follow-up was 68.2 months. Among MLH1 mutation carriers, mutations in MLH1 were associated with colorectal cancer in 249 (61%) of 409 men and women; endometrial cancer in 53 of 196 (27%) women; and ovarian cancer in 15 (8%) of 196 women. Among MSH2 mutation carriers, mutations in MSH2 (the most prevalent mutations overall) were most commonly associated with female-specific cancers: endometrial cancer in 83 (30%) of 279 women; ovarian cancer in 28 (10%) of 279 women; and colorectal cancer in 239 (50%) 479 men and women. Mutations in MSH6 were less prevalent, and MSH6 mutation carriers presented with colorectal and endometrial cancer at later ages than carriers of mutations in MSH2 or MLH1. When stratified by mutation type, women with truncating MLH1 mutations had later ages of onset of endometrial cancer than those with nontruncating mutations (median difference, 6.6 years; 95% CI, 2.7-10.4; P = .002). Carriers of truncating MLH1 mutations presented with colorectal cancer at later ages than those with other mutations, but the difference was not statistically significant.
Individuals with known Lynch syndrome could be risk stratified by mutated gene and mutation type in tailored surveillance programs. Specifically, individuals with MSH6 mutations could be offered cancer surveillance from a later age. Furthermore, those with truncating MLH1 mutations could begin endometrial cancer surveillance later than those with nontruncating mutations.
林奇综合征是由显性遗传的种系突变引起的,通过细胞错配修复系统的失活,使个体易患结直肠、子宫内膜、卵巢和其他癌症。林奇综合征相关的癌症可以通过监测策略来治疗,这可能会提高生存率。开始监测的年龄存在争议。
确定突变基因和突变类型是否会影响林奇综合征相关癌症的发病年龄。
设计、地点和参与者:这是一项对在英国西北部一家大型四级基因组医学转诊中心的临床数据库中记录有林奇综合征相关结直肠、子宫内膜和/或卵巢癌的个体进行的回顾性队列研究。
突变基因(MLH1、MSH2、MSH6 和/或 PMS2)和突变类型(截断、剪接或大片段重排)。
癌症诊断时的年龄。
共纳入 1063 名经证实的林奇综合征患者,其中男性 495 名,女性 568 名(平均年龄 52 岁;年龄范围为 10-93 岁[数据库中包括儿童,但没有儿童患癌症])。546 名男性和女性患有结直肠癌,162 名女性患有子宫内膜癌,49 名女性患有卵巢癌;中位随访时间为 68.2 个月。在 MLH1 突变携带者中,MLH1 中的突变与 409 名男性和女性中的 249 例(61%)结直肠癌相关;196 名女性中的 53 例(27%)子宫内膜癌;196 名女性中的 15 例(8%)卵巢癌。在 MSH2 突变携带者中,MSH2 中的突变(总体上最常见的突变)最常与女性特异性癌症相关:279 名女性中的 83 例(30%)子宫内膜癌;279 名女性中的 28 例(10%)卵巢癌;479 名男性和女性中的 239 例(50%)结直肠癌。MSH6 突变较少见,携带 MSH6 突变的患者比携带 MSH2 或 MLH1 突变的患者发病年龄更大。按突变类型分层时,携带截断 MLH1 突变的女性子宫内膜癌发病年龄晚于非截断突变者(中位数差异,6.6 岁;95%CI,2.7-10.4;P = .002)。携带截断 MLH1 突变的患者比其他突变者结直肠癌发病年龄更大,但差异无统计学意义。
已知患有林奇综合征的个体可根据突变基因和突变类型进行风险分层,以制定个体化的监测方案。具体来说,MSH6 突变携带者可以在较晚的年龄接受癌症监测。此外,携带截断 MLH1 突变的患者比携带非截断突变的患者开始子宫内膜癌监测的年龄更晚。