Ammann Eric M, Shanafelt Tait D, Larson Melissa C, Wright Kara B, McDowell Bradley D, Link Brian K, Chrischilles Elizabeth A
Department of Epidemiology, College of Public Health, University of Iowa, Iowa City, IA; Holden Comprehensive Cancer Center, University of Iowa, Iowa City, IA.
Department of Internal Medicine, Mayo Clinic, Rochester, MN.
Clin Lymphoma Myeloma Leuk. 2017 Dec;17(12):e11-e25. doi: 10.1016/j.clml.2017.07.004. Epub 2017 Jul 19.
Novel targeted therapies offer excellent short-term outcomes in patients with chronic lymphocytic leukemia and small lymphocytic lymphoma (CLL/SLL). However, there is disagreement over how widely these therapies should be used in place of standard chemo-immunotherapy (CIT). We investigated whether stratification on the length of the interval between first-line (T1) and second-line (T2) treatments could identify a subgroup of older patients with relapsed CLL/SLL with an expectation of normal overall survival, and for whom CIT could be an acceptable treatment choice.
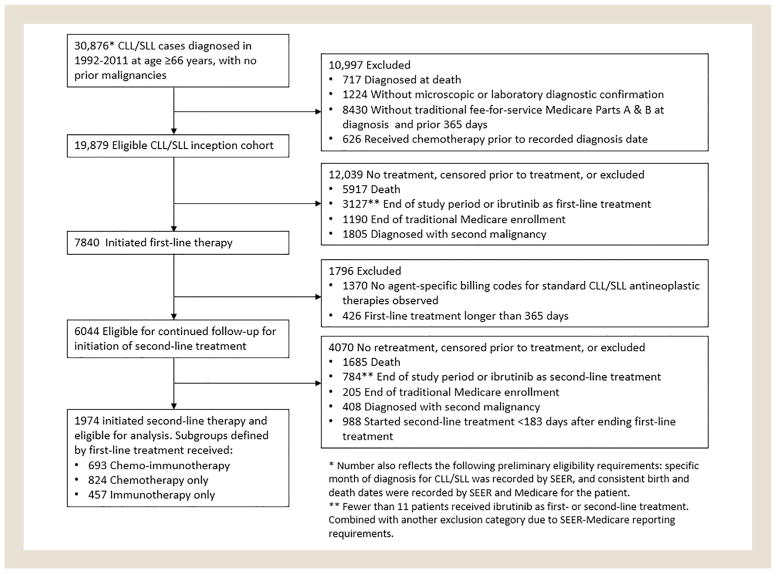
Patients with relapsed CLL/SLL who received T2 were identified from the SEER-Medicare Linked Database. Five-year relative survival (RS5; ie, the ratio of observed survival to expected survival based on population life tables) was assessed after stratifying patients on the interval between T1 and T2. We then validated our findings in the Mayo Clinic CLL Database.
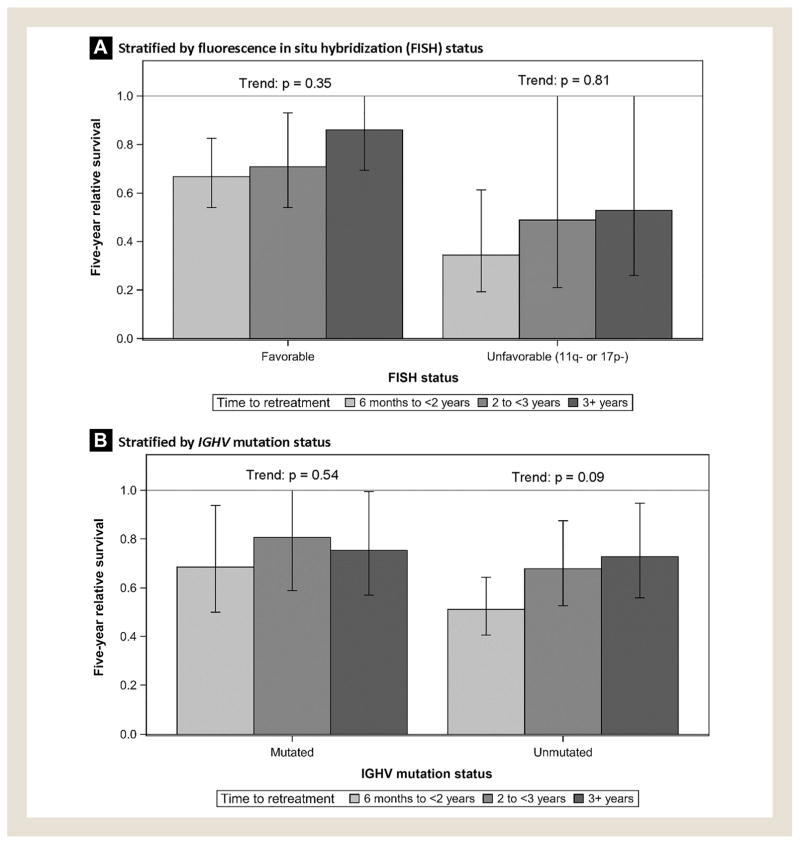
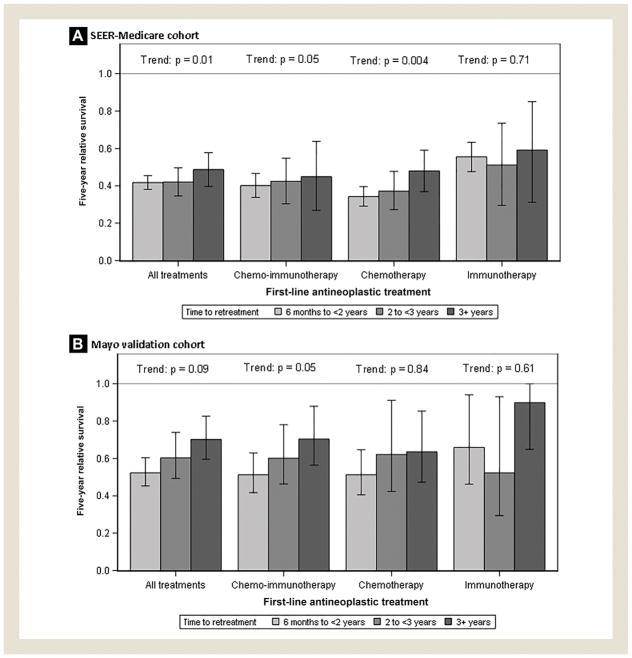
Among 1974 SEER-Medicare patients (median age = 77 years) who received T2 for relapsed CLL/SLL, longer time-to-retreatment was associated with a modestly improved prognosis (P = .01). However, even among those retreated ≥ 3 years after T1, survival was poor compared with the general population (RS5 = 0.50 or lower in SEER-Medicare). Similar patterns were observed in the younger Mayo validation cohort, although prognosis was better overall among the Mayo patients, and patients with favorable fluorescence in situ hybridization retreated ≥ 3 years after T1 had close to normal expected survival (RS5 = 0.87).
Further research is needed to quantify the degree to which targeted therapies provide meaningful improvements over CIT in long-term outcomes for older patients with relapsed CLL/SLL.
新型靶向疗法在慢性淋巴细胞白血病和小淋巴细胞淋巴瘤(CLL/SLL)患者中具有出色的短期疗效。然而,对于这些疗法应在多大程度上广泛替代标准化学免疫疗法(CIT)存在分歧。我们研究了根据一线(T1)和二线(T2)治疗之间的间隔时间进行分层,是否能够识别出一组复发CLL/SLL的老年患者,他们有望获得正常的总生存期,并且CIT可能是一种可接受的治疗选择。
从SEER - 医疗保险链接数据库中识别出接受T2治疗的复发CLL/SLL患者。在根据T1和T2之间的间隔对患者进行分层后,评估五年相对生存率(RS5;即观察到的生存率与基于人群生命表的预期生存率之比)。然后我们在梅奥诊所CLL数据库中验证了我们的发现。
在1974例接受T2治疗的复发CLL/SLL的SEER - 医疗保险患者(中位年龄 = 77岁)中,较长的再治疗时间与适度改善的预后相关(P = 0.01)。然而,即使在T1后≥3年接受再治疗的患者中,与一般人群相比生存率仍较差(SEER - 医疗保险中的RS5 = 0.50或更低)。在较年轻的梅奥验证队列中观察到类似模式,尽管梅奥患者的总体预后较好,并且T1后≥3年接受再治疗的具有良好荧光原位杂交结果的患者预期生存率接近正常(RS5 = 0.87)。
需要进一步研究以量化靶向疗法在复发CLL/SLL老年患者的长期结局方面比CIT提供有意义改善的程度。