Cerva C, Maffongelli G, Svicher V, Salpini R, Colagrossi L, Battisti A, Mariotti B, Cerretti R, Cudillo L, Sarmati L
Clinical Infectious Disease, Department of Systems Medicine, Tor Vergata University, Rome, Italy.
Department of Experimental Medicine and Surgery, Tor Vergata University, Rome, Italy.
BMC Infect Dis. 2017 Aug 15;17(1):566. doi: 10.1186/s12879-017-2672-6.
HBV reactivation is associated with high mortality rates in hematopoietic stem cell transplantation (HSCT) and prophylactic lamivudine (LMV) treatment is suggested to prevent this phenomenon. However, the duration of LMV treatment in HSCT patients is not fully defined and the time of immune recovery is considered the best parameter for a drug to be safely interrupted. In patients undergoing allogeneic HSCT, the time of immune recovery is not easy to define and may take years after transplantation and prolonged LMV treatments, which can lead to drug-resistant viral strains.
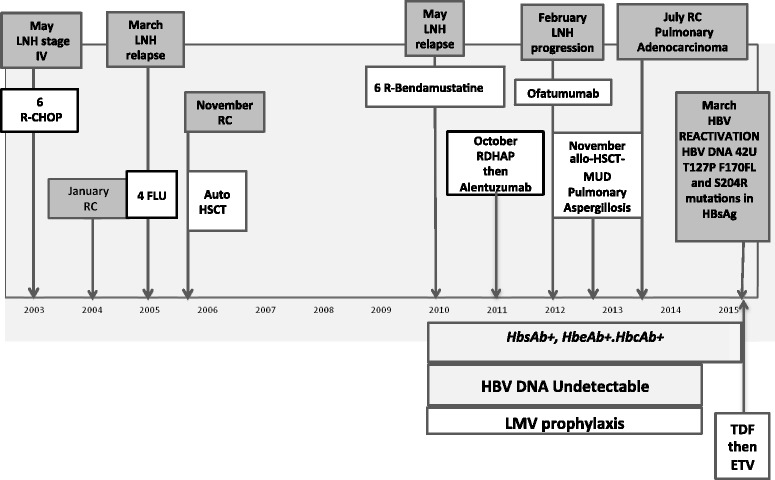
An anti-HBc-positive hematological patient who was undergoing prolonged immunosuppression and who experienced HBV reactivation 3 months after the suspension of a prolonged LMV prophylaxis is described. HBV-DNA matching an atypical serological profile characterized by HbsAg negativity and anti-HBs positivity was detected in the patient. The genotypic analysis of the HBV strain identified T127P, F170FL and S204R mutations of HbsAg, which can hinder HBsAg recognition in a diagnostic assay.
HBV reactivation in the HSCT host can be sustained by HBsAg viral variants with characteristics of altered immunogenicity that cannot be detected by usual laboratory tests. This clinical case description suggests the importance of screening for serum HBV-DNA levels in the diagnosis of HBV reactivation and monitoring HBV-DNA after prophylaxis suspension, particularly in HSCT subjects who have undergone prolonged periods of LMV treatment.
乙肝病毒再激活与造血干细胞移植(HSCT)的高死亡率相关,建议使用拉米夫定(LMV)进行预防性治疗以预防这种现象。然而,HSCT患者中LMV治疗的持续时间尚未完全确定,免疫恢复时间被认为是安全中断药物治疗的最佳参数。在接受异基因HSCT的患者中,免疫恢复时间不易确定,移植后可能需要数年时间,且LMV治疗时间延长,这可能导致耐药病毒株的产生。
描述了一名抗-HBc阳性的血液学患者,该患者正在接受长期免疫抑制治疗,在长期LMV预防治疗中断3个月后发生了乙肝病毒再激活。在该患者中检测到乙肝病毒DNA,其血清学特征为HbsAg阴性和抗-HBs阳性,属于非典型血清学特征。对乙肝病毒株的基因分析确定了HbsAg的T127P、F170FL和S204R突变,这些突变可能会在诊断检测中阻碍HbsAg的识别。
HSCT宿主中的乙肝病毒再激活可能由具有免疫原性改变特征的HbsAg病毒变异体维持,这些变异体无法通过常规实验室检测检测到。该临床病例描述表明,在乙肝病毒再激活的诊断中筛查血清乙肝病毒DNA水平以及在预防治疗中断后监测乙肝病毒DNA的重要性,特别是在接受了长期LMV治疗的HSCT患者中。