Al Therwani Safa, Malmberg My Emma Sofie, Rosenbaek Jeppe Bakkestroem, Bech Jesper Noergaard, Pedersen Erling Bjerregaard
University Clinic in Nephrology and Hypertension, Department of Medical Research, Holstebro Hospital and Aarhus University, Hospital Unit Jutland West, Laegaardvej 12, 7500, Holstebro, Denmark.
BMC Nephrol. 2017 Aug 15;18(1):268. doi: 10.1186/s12882-017-0686-3.
Tolvaptan slows progression of autosomal dominant polycystic kidney disease (ADPKD) by antagonizing the vasopressin-cAMP axis. Nitric oxide (NO) stimulates natriuresis and diuresis, but its role is unknown during tolvaptan treatment in ADPKD.
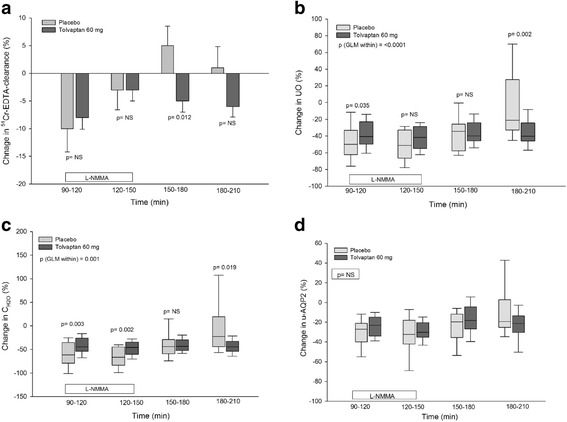
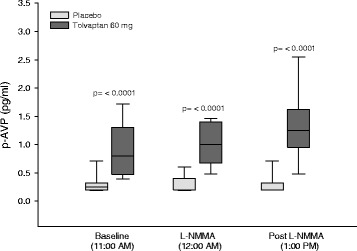
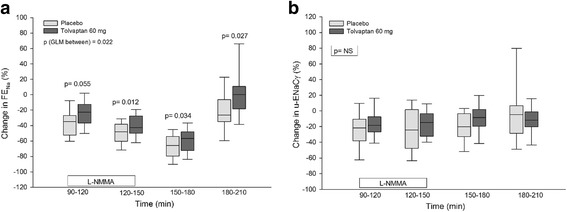
Eighteen patients with ADPKD received tolvaptan 60 mg or placebo in a randomized, placebo-controlled, double blind, crossover study. L-NMMA (L-NG-monomethyl-arginine) was given as a bolus followed by continuous infusion during 60 min. We measured: GFR, urine output (UO), free water clearance (C), fractional excretion of sodium (FE), urinary excretion of aquaporin-2 channels (u-AQP2) and epithelial sodium channels (u-ENaCγ), plasma concentrations of vasopressin (p-AVP), renin (PRC), angiotensinII (p-AngII), aldosterone (p-Aldo), and central blood pressure (cBP).
During tolvaptan with NO-inhibition, a more pronounced decrease was measured in UO, C (61% vs 43%) and FE (46% vs 41%) after placebo than after tolvaptan; GFR and u-AQP2 decreased to the same extent; p-AVP increased three fold, whereas u-ENaC, PRC, p-AngII, and p-Aldo remained unchanged. After NO-inhibition, GFR increased after placebo and remained unchanged after tolvaptan (5% vs -6%). Central diastolic BP (CDBP) increased to a higher level after placebo than tolvaptan. Body weight fell during tolvaptan treatment.
During NO inhibition, tolvaptan antagonized both the antidiuretic and the antinatriuretic effect of L-NMMA, partly via an AVP-dependent mechanism. U-AQP2 was not changed by tolvaptan, presumeably due to a counteracting effect of elevated p-AVP. The reduced GFR during tolvaptan most likely is caused by the reduction in extracellular fluid volume and blood pressure.
Clinical Trial no: NCT02527863 . Registered 18 February 2015.
托伐普坦通过拮抗血管加压素 - cAMP轴来减缓常染色体显性多囊肾病(ADPKD)的进展。一氧化氮(NO)可刺激尿钠排泄和利尿,但在ADPKD患者接受托伐普坦治疗期间其作用尚不清楚。
在一项随机、安慰剂对照、双盲、交叉研究中,18例ADPKD患者接受60mg托伐普坦或安慰剂治疗。静脉推注L - NMMA(L - NG - 单甲基精氨酸),随后在60分钟内持续输注。我们测量了:肾小球滤过率(GFR)、尿量(UO)、自由水清除率(C)、钠分数排泄率(FE)、水通道蛋白 - 2通道的尿排泄量(u - AQP2)和上皮钠通道(u - ENaCγ)、血管加压素(p - AVP)、肾素(PRC)、血管紧张素II(p - AngII)、醛固酮(p - Aldo)的血浆浓度以及中心血压(cBP)。
在托伐普坦联合NO抑制治疗期间,与托伐普坦治疗后相比,安慰剂治疗后UO、C(61%对43%)和FE(46%对41%)的下降更为明显;GFR和u - AQP2下降程度相同;p - AVP增加了三倍,而u - ENaC、PRC、p - AngII和p - Aldo保持不变。NO抑制后,安慰剂治疗后GFR升高,托伐普坦治疗后保持不变(5%对 - 6%)。安慰剂治疗后中心舒张压(CDBP)升高幅度高于托伐普坦治疗后。托伐普坦治疗期间体重下降。
在NO抑制期间,托伐普坦部分通过AVP依赖机制拮抗了L - NMMA的抗利尿和抗尿钠排泄作用。托伐普坦未改变u - AQP2,推测是由于p - AVP升高的抵消作用。托伐普坦治疗期间GFR降低很可能是由于细胞外液量和血压降低所致。
临床试验编号:NCT02527863。于2015年2月18日注册。