International Health Policy Program, Ministry of Public Health, Nonthaburi, Thailand.
Int J Health Policy Manag. 2017 Feb 1;6(2):107-110. doi: 10.15171/ijhpm.2016.99.
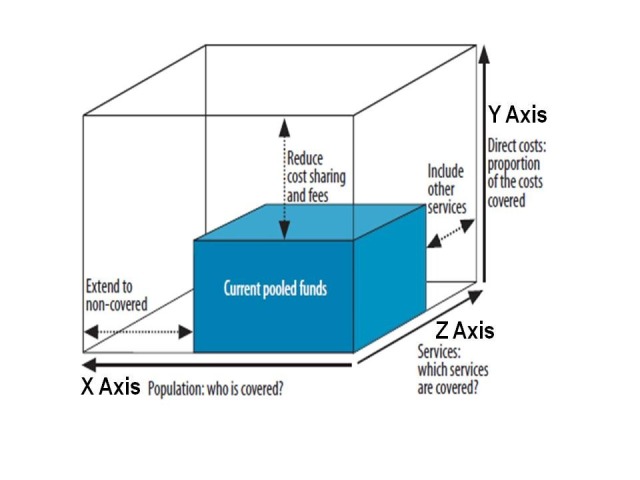
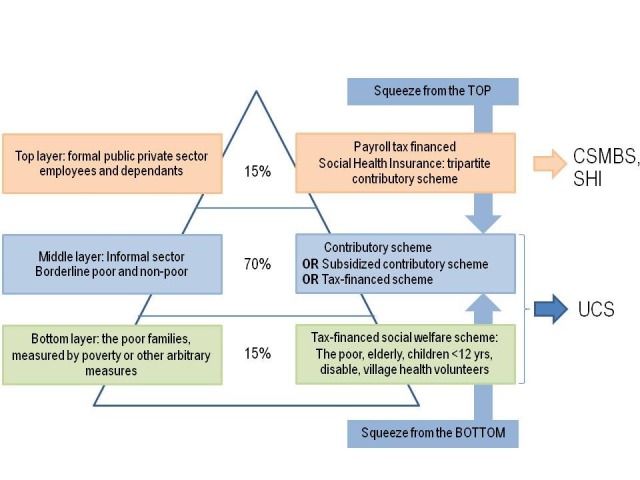
In responses to Norheim's editorial, this commentary offers reflections from Thailand, how the five unacceptable trade-offs were applied to the universal health coverage (UHC) reforms between 1975 and 2002 when the whole 64 million people were covered by one of the three public health insurance systems. This commentary aims to generate global discussions on how best UHC can be gradually achieved. Not only the proposed five discrete trade-offs within each dimension, there are also trade-offs between the three dimensions of UHC such as population coverage, service coverage and cost coverage. Findings from Thai UHC show that equity is applied for the population coverage extension, when the low income households and the informal sector were the priority population groups for coverage extension by different prepayment schemes in 1975 and 1984, respectively. With an exception of public sector employees who were historically covered as part of fringe benefits were covered well before the poor. The private sector employees were covered last in 1990. Historically, Thailand applied a comprehensive benefit package where a few items are excluded using the negative list; until there was improved capacities on technology assessment that cost-effectiveness are used for the inclusion of new interventions into the benefit package. Not only cost-effectiveness, but long term budget impact, equity and ethical considerations are taken into account. Cost coverage is mostly determined by the fiscal capacities. Close ended budget with mix of provider payment methods are used as a tool for trade-off service coverage and financial risk protection. Introducing copayment in the context of fee-for-service can be harmful to beneficiaries due to supplier induced demands, inefficiency and unpredictable out of pocket payment by households. UHC achieves favorable outcomes as it was implemented when there was a full geographical coverage of primary healthcare coverage in all districts and sub-districts after three decade of health infrastructure investment and health workforce development since 1980s. The legacy of targeting population group by different prepayment mechanisms, leading to fragmentation, discrepancies and inequity across schemes, can be rectified by harmonization at the early phase when these schemes were introduced. Robust public accountability and participation mechanisms are recommended when deciding the UHC strategy.
针对诺海姆的社论,本文从泰国的角度进行了反思,即 1975 年至 2002 年期间,在三种公共医疗保险体系覆盖了全体 6400 万人的情况下,全民健康覆盖(UHC)改革中如何应用了五个不可接受的权衡取舍。本文旨在引发关于如何逐步实现全民健康覆盖的全球讨论。不仅要考虑到每个维度中提出的五个离散权衡取舍,还要考虑到全民健康覆盖的三个维度(人口覆盖、服务覆盖和费用覆盖)之间的权衡取舍。泰国全民健康覆盖的经验表明,在 1975 年和 1984 年,通过不同的预付款方案,将低收入家庭和非正规部门作为优先覆盖群体,实现了人口覆盖的扩大,这体现了公平性。除了历史上作为福利的一部分覆盖的公共部门员工外,穷人之前的覆盖范围要广。私营部门员工最后在 1990 年被覆盖。泰国历史上应用了综合福利套餐,只使用负面清单排除了少数项目;直到有了更好的技术评估能力,才将成本效益纳入了福利套餐中。不仅考虑了成本效益,还考虑了长期预算影响、公平性和伦理考虑。费用覆盖主要由财政能力决定。采用封闭式预算和混合提供者支付方式,作为权衡服务覆盖范围和财务风险保护的工具。在按服务收费的背景下引入共付额,可能会因供方诱导需求、效率低下以及家庭不可预测的自付费用而对受益人造成伤害。全民健康覆盖实现了有利的结果,因为它是在经过 30 年的卫生基础设施投资和 20 世纪 80 年代以来的卫生人力发展之后,在所有地区和分区实现了初级卫生保健全覆盖的背景下实施的。通过不同的预付款机制针对特定人群进行定位的做法导致了不同计划之间的碎片化、差异和不公平,这些问题可以在这些计划引入的早期阶段通过协调加以纠正。建议在决定全民健康覆盖战略时,建立健全的公共问责和参与机制。