Pienaar Elsje, Sarathy Jansy, Prideaux Brendan, Dietzold Jillian, Dartois Véronique, Kirschner Denise E, Linderman Jennifer J
Department of Chemical Engineering, University of Michigan, Ann Arbor, Michigan, United States of America.
Department of Microbiology and Immunology, University of Michigan Medical School, Ann Arbor, Michigan, United States of America.
PLoS Comput Biol. 2017 Aug 17;13(8):e1005650. doi: 10.1371/journal.pcbi.1005650. eCollection 2017 Aug.
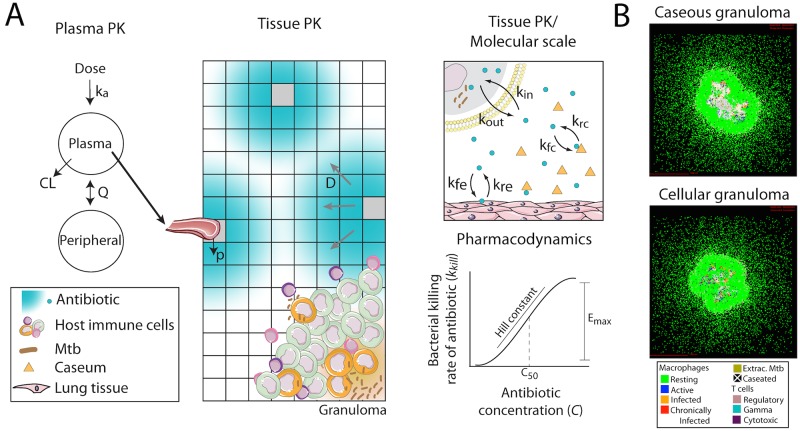
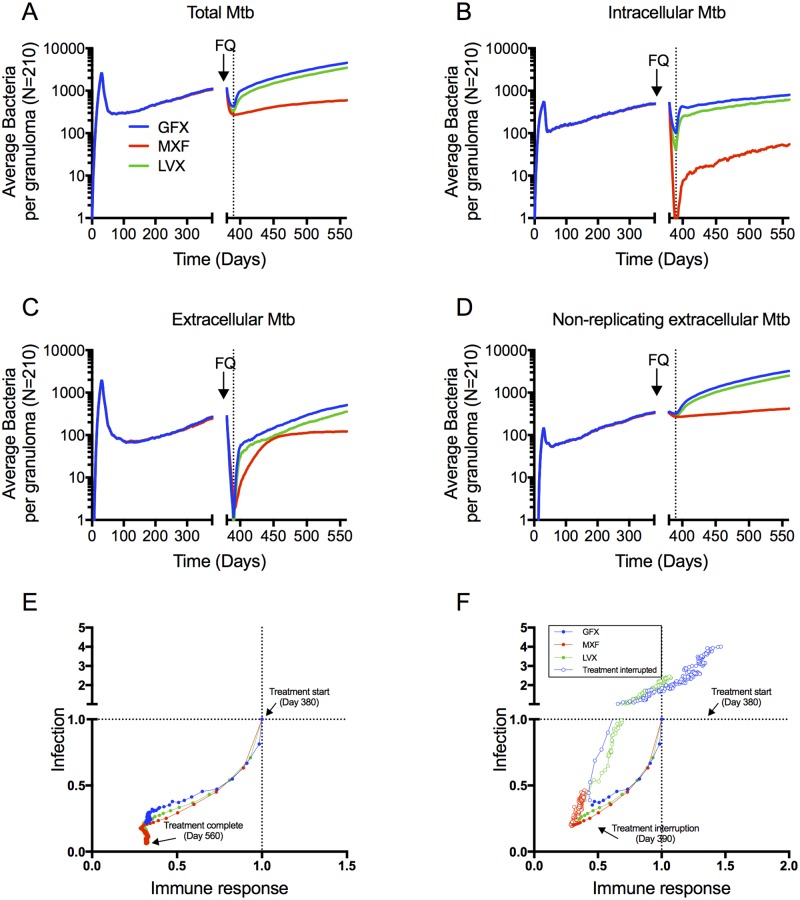
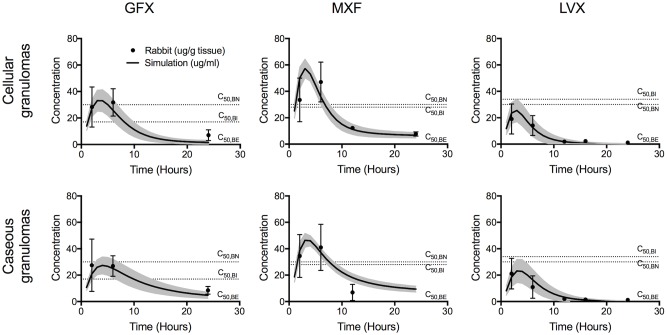
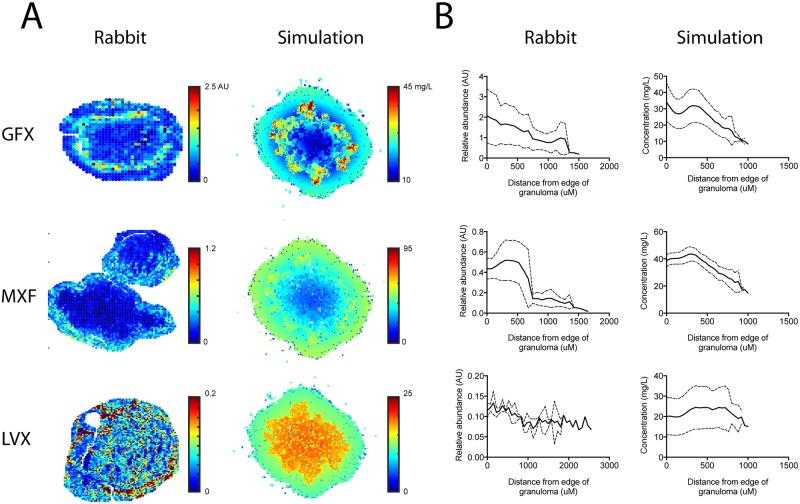
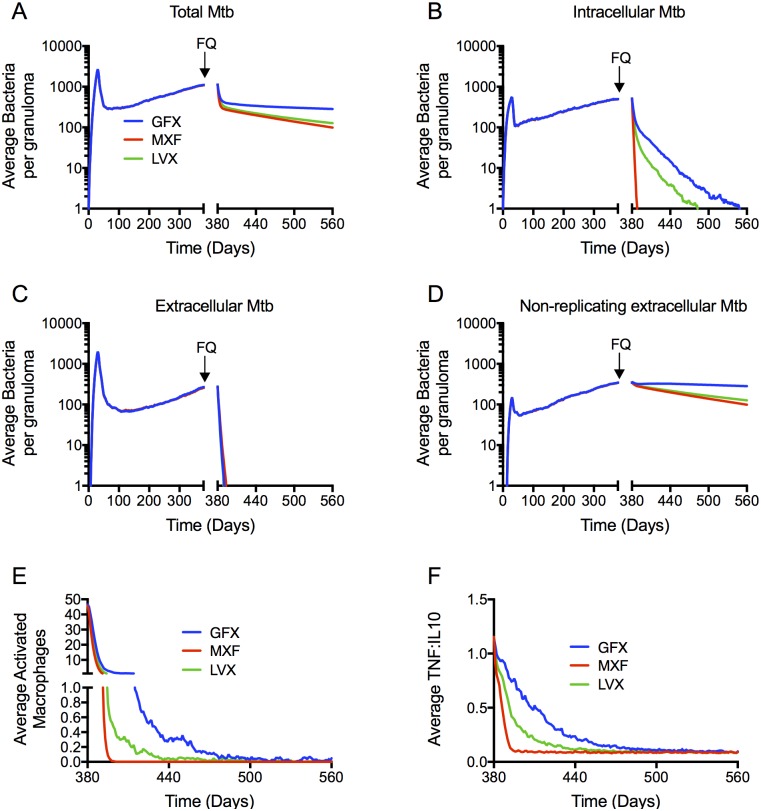
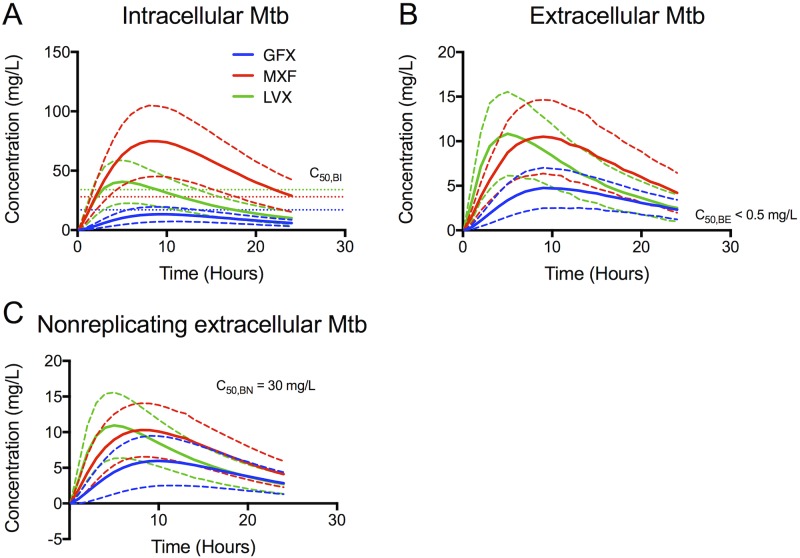
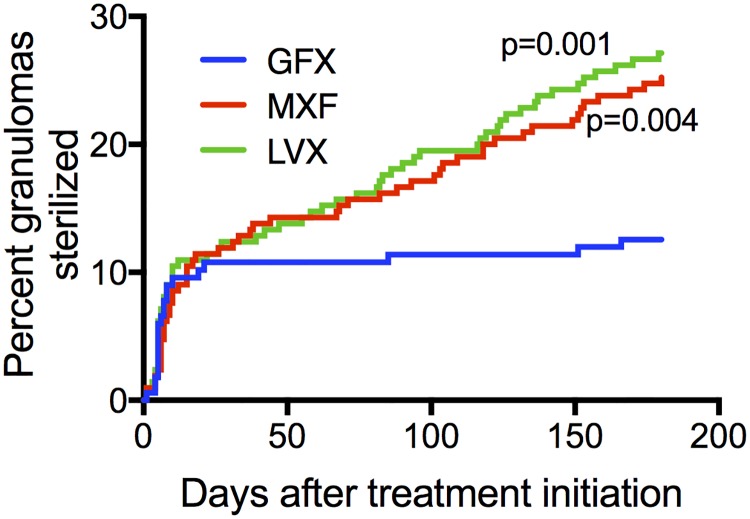
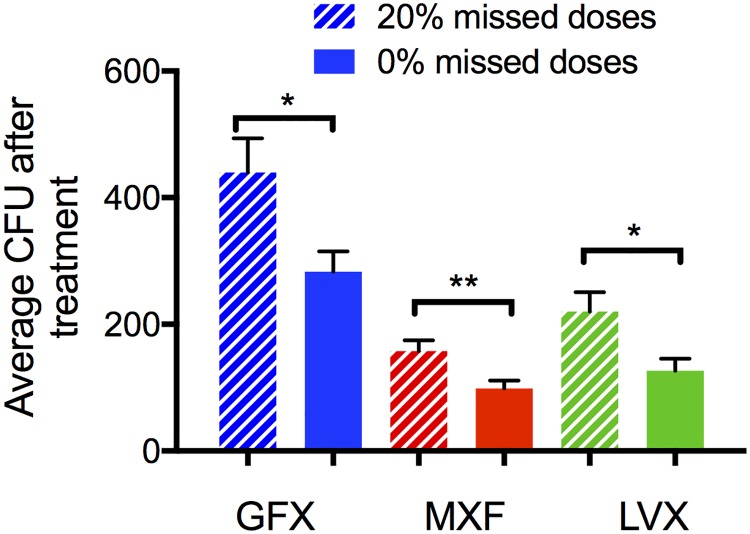
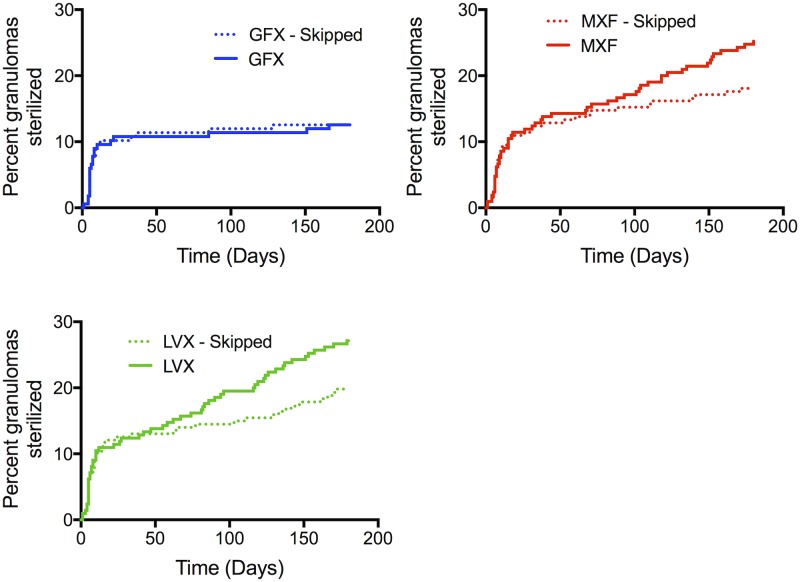
Granulomas are complex lung lesions that are the hallmark of tuberculosis (TB). Understanding antibiotic dynamics within lung granulomas will be vital to improving and shortening the long course of TB treatment. Three fluoroquinolones (FQs) are commonly prescribed as part of multi-drug resistant TB therapy: moxifloxacin (MXF), levofloxacin (LVX) or gatifloxacin (GFX). To date, insufficient data are available to support selection of one FQ over another, or to show that these drugs are clinically equivalent. To predict the efficacy of MXF, LVX and GFX at a single granuloma level, we integrate computational modeling with experimental datasets into a single mechanistic framework, GranSim. GranSim is a hybrid agent-based computational model that simulates granuloma formation and function, FQ plasma and tissue pharmacokinetics and pharmacodynamics and is based on extensive in vitro and in vivo data. We treat in silico granulomas with recommended daily doses of each FQ and compare efficacy by multiple metrics: bacterial load, sterilization rates, early bactericidal activity and efficacy under non-compliance and treatment interruption. GranSim reproduces in vivo plasma pharmacokinetics, spatial and temporal tissue pharmacokinetics and in vitro pharmacodynamics of these FQs. We predict that MXF kills intracellular bacteria more quickly than LVX and GFX due in part to a higher cellular accumulation ratio. We also show that all three FQs struggle to sterilize non-replicating bacteria residing in caseum. This is due to modest drug concentrations inside caseum and high inhibitory concentrations for this bacterial subpopulation. MXF and LVX have higher granuloma sterilization rates compared to GFX; and MXF performs better in a simulated non-compliance or treatment interruption scenario. We conclude that MXF has a small but potentially clinically significant advantage over LVX, as well as LVX over GFX. We illustrate how a systems pharmacology approach combining experimental and computational methods can guide antibiotic selection for TB.
肉芽肿是复杂的肺部病变,是结核病(TB)的标志。了解肺部肉芽肿内的抗生素动态对于改善和缩短漫长的结核病治疗疗程至关重要。三种氟喹诺酮类药物(FQs)通常作为耐多药结核病治疗的一部分被开具处方:莫西沙星(MXF)、左氧氟沙星(LVX)或加替沙星(GFX)。迄今为止,尚无足够的数据支持选择一种氟喹诺酮类药物而非另一种,也无法表明这些药物在临床上是等效的。为了预测MXF、LVX和GFX在单个肉芽肿水平上的疗效,我们将计算建模与实验数据集整合到一个单一的机制框架GranSim中。GranSim是一种基于混合智能体的计算模型,可模拟肉芽肿的形成和功能、氟喹诺酮类药物的血浆和组织药代动力学及药效学,且基于广泛的体外和体内数据。我们用每种氟喹诺酮类药物的推荐日剂量对虚拟肉芽肿进行处理,并通过多种指标比较疗效:细菌载量、杀菌率、早期杀菌活性以及在不依从和治疗中断情况下的疗效。GranSim再现了这些氟喹诺酮类药物的体内血浆药代动力学、时空组织药代动力学和体外药效学。我们预测,MXF比LVX和GFX更快地杀死细胞内细菌,部分原因是其细胞蓄积率更高。我们还表明,所有三种氟喹诺酮类药物都难以杀灭存在于干酪样物质中的非复制细菌。这是由于干酪样物质内的药物浓度适中,而该细菌亚群的抑制浓度较高。与GFX相比,MXF和LVX具有更高的肉芽肿杀菌率;并且在模拟的不依从或治疗中断情况下,MXF表现更好。我们得出结论,MXF相对于LVX有微小但可能具有临床意义的优势,LVX相对于GFX也是如此。我们说明了一种结合实验和计算方法的系统药理学方法如何能够指导结核病的抗生素选择。