Bárta Jiří, Brát Radim
Cardiac Surgery, University Hospital Ostrava, 17.listopadu 1790, 708 52, Ostrava-Poruba, Czech Republic.
J Cardiothorac Surg. 2017 Aug 17;12(1):69. doi: 10.1186/s13019-017-0625-1.
The aim of our study was to investigate, whether enhancement of left atrial cryoablation by ablation of the autonomic nervous system of left atrium leads to influencing the outcomes of surgical treatment of atrial fibrillation in patients with structural heart disease undergoing open-heart surgery.
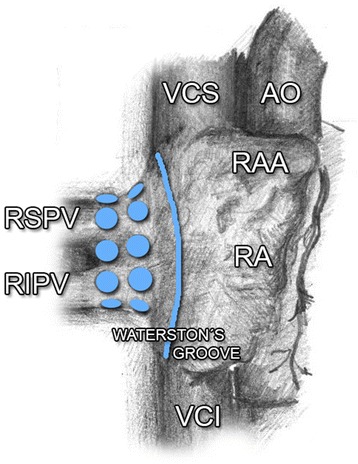
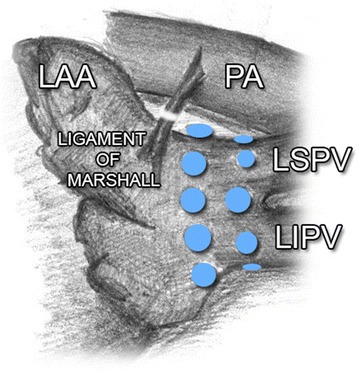
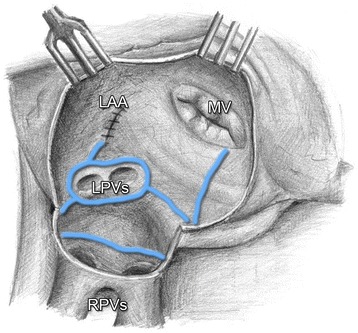
The observed patient file consisted of 100 patients, who have undergone a combined open-heart surgery at our department between July 2012 and December 2014. The patients were indicated for the surgical procedure due to structural heart disease, and suffered from paroxysmal, persistent, or long-standing persistent atrial fibrillation. In all cases, left atrial cryoablation was performed in the extent of isolation of pulmonary veins, box lesion, connecting lesion with mitral annulus, amputation of the left atrial appendage and connecting lesion of the appendage base with left pulmonary veins. Furthermore, 35 of the patients underwent mapping and radiofrequency ablation of ganglionated plexi, together with discision and ablation of the ligament of Marshall (Group GP). A control group was consisted of 65 patients without ganglionated plexi intervention (Group LA). The main primary outcome was establishment and duration of sinus rhythm in the course of one-year follow-up.
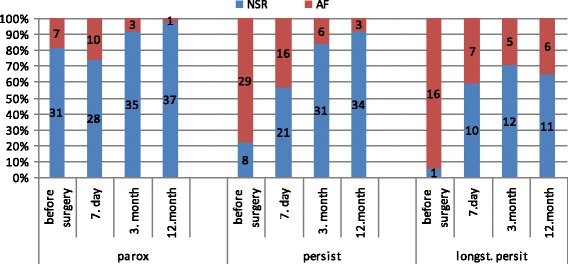
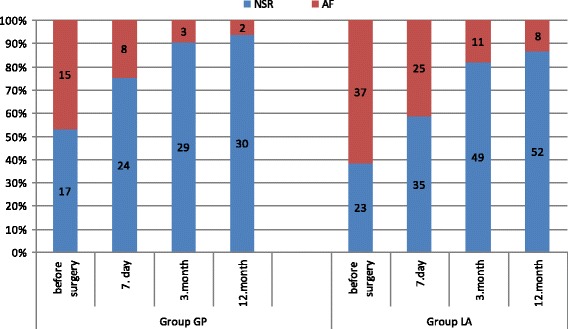
Evaluation of the number of patients with a normal sinus rhythm in per cent has shown comparable values in both groups (Group GP - 93.75%, Group LA - 86.67%, p = 0.485); comparable results were also observed in patients with normal sinus rhythm without anti-arrhythmic treatment in the 12th month (Group GP - 50%, Group LA - 47%, p = 0.306). We have not observed any relation between the recurrence of atrial fibrillation and the presence of a mitral valve surgery, or between the presence of a mitral and tricuspid valves surgery and between the left atrial diameter > 50 mm.
Enhancement of left atrial cryoablation by gangionated plexi ablation did not influence the outcomes of surgical ablation due to atrial fibrillation in our population in the course of 12-month follow-up.
The study was approved retrospectively by the Ethics Committee of the University Hospital Ostrava ( reference number 867/2016).
我们研究的目的是调查,通过消融左心房自主神经系统来增强左心房冷冻消融是否会影响接受心脏直视手术的结构性心脏病患者的心房颤动外科治疗结果。
观察的患者资料包括100例于2012年7月至2014年12月在我们科室接受心脏直视联合手术的患者。这些患者因结构性心脏病而接受手术,患有阵发性、持续性或长期持续性心房颤动。所有病例均进行了肺静脉隔离、盒状病变、与二尖瓣环连接病变、左心耳切除术以及心耳基部与左肺静脉连接病变范围内的左心房冷冻消融。此外,35例患者接受了神经节丛的标测和射频消融,以及Marshall韧带的切断和消融(GP组)。对照组由65例未进行神经节丛干预的患者组成(LA组)。主要的主要结局是在一年随访期间窦性心律的建立和持续时间。
对窦性心律正常患者百分比的评估显示两组值相当(GP组 - 93.75%,LA组 - 86.67%,p = 0.485);在第12个月未接受抗心律失常治疗的窦性心律正常患者中也观察到了类似结果(GP组 - 50%,LA组 - 47%,p = 0.306)。我们未观察到心房颤动复发与二尖瓣手术的存在之间、二尖瓣和三尖瓣手术的存在之间以及左心房直径>50mm之间存在任何关联。
在我们的研究人群中,在12个月的随访期间,通过神经节丛消融增强左心房冷冻消融并未影响因心房颤动进行的外科消融结果。
该研究经俄斯特拉发大学医院伦理委员会回顾性批准(参考编号867/2016)。