Yuan Shu-Qiang, Nie Run-Cong, Chen Shi, Chen Xiao-Jiang, Chen Yong-Ming, Xu Li-Pu, Yang Li-Fang, Zhou Zhi-Wei, Peng Jun-Sheng, Chen Ying-Bo
Sun Yat-sen University Cancer Center; State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine, Guangzhou, China.
Department of Gastric Surgery, the 6th Affiliated Hospital, Sun Yat-sen University, Guangzhou, China.
J Cancer. 2017 Jul 20;8(12):2231-2237. doi: 10.7150/jca.18932. eCollection 2017.
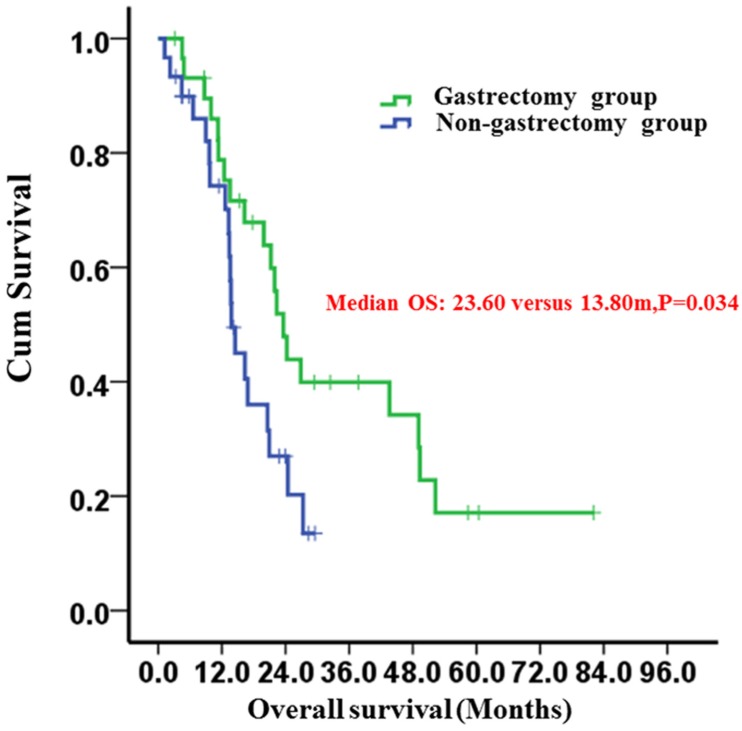
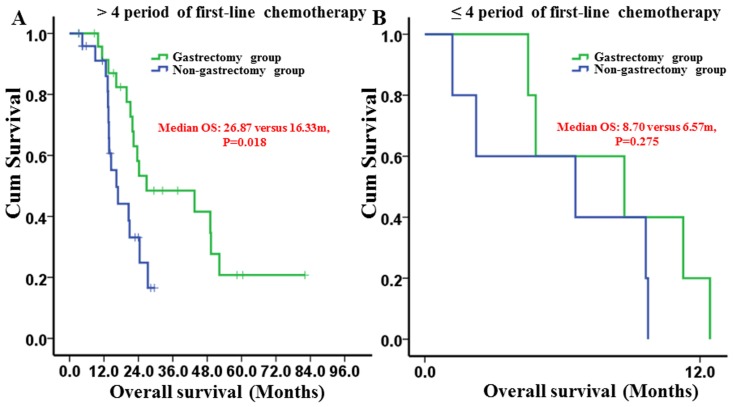
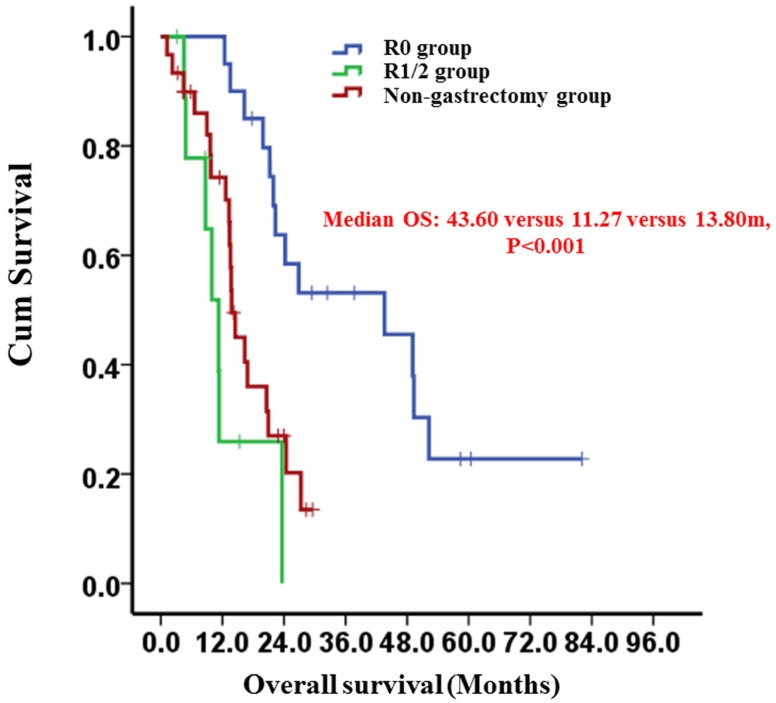
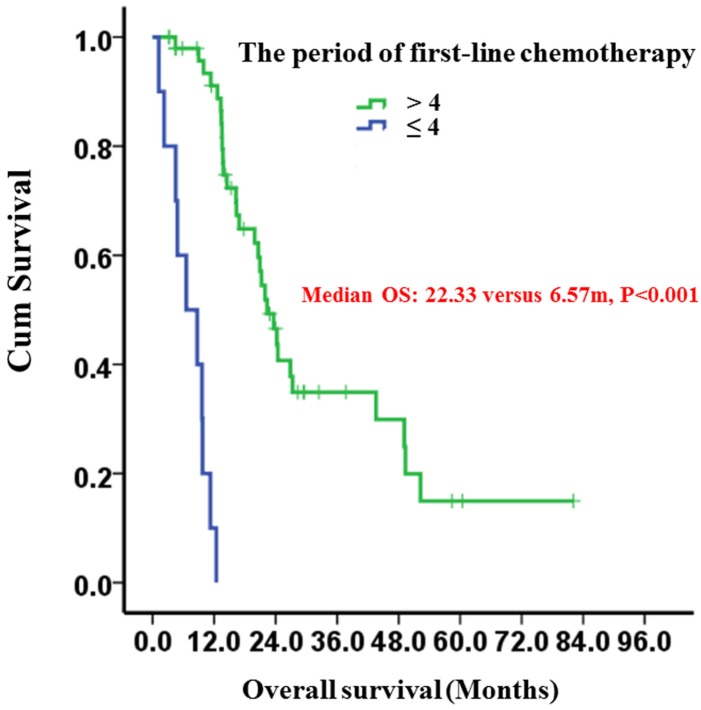
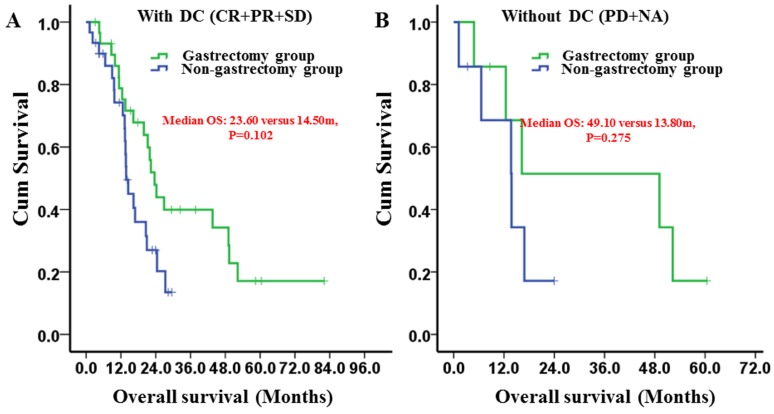
The present study aimed to explore whether gastric cancer patients with peritoneal seeding after receiving palliative chemotherapy could benefit from gastrectomy and to identify patients with peritoneal seeding who should be selected to receive gastrectomy. A total of 201 gastric cancer patients were diagnosed with peritoneal seeding and received palliative chemotherapy. Propensity score matching (PSM) was performed to balance the selection bias. After PSM, compared with non-gastrectomy group, gastrectomy group had a longer median overall survival (OS) (23.60 vs. 13.80 moths; P=0.034). Patients with R0 resection had a median OS of 43.60 months compared with 11.27 months in patients who underwent R1/2 resection (P<0.001). The median OS times between the R1/2 resection and non-gastrectomy groups were not different (P=0.139). Subgroup analysis revealed that only patients receiving more than 4 periods of first-line chemotherapy benefited from gastrectomy (P=0.018), whereas patients receiving 1-4 periods of first-line chemotherapy did not (P=0.275). Multivariate analysis showed that gastrectomy (P=0.012) and the period of first-line chemotherapy (P<0.001) were independent prognostic factors. The overall postoperative morbidity was 3.03% (1/33) in the gastrectomy group, and no treatment-related death was observed. The present study indicated that gastrectomy after palliative chemotherapy is a safe procedure and showed a survival benefit for gastric cancer patients with peritoneal seeding. Moreover, clinically curative R0 gastrectomy and more than 4 periods of palliative chemotherapy resulted in better clinical outcomes.
本研究旨在探讨接受姑息化疗后出现腹膜种植的胃癌患者是否能从胃切除术中获益,并确定应选择接受胃切除术的腹膜种植患者。共有201例被诊断为腹膜种植的胃癌患者接受了姑息化疗。进行倾向评分匹配(PSM)以平衡选择偏倚。PSM后,与未行胃切除术组相比,胃切除术组的中位总生存期(OS)更长(23.60个月对13.80个月;P = 0.034)。R0切除患者的中位OS为43.60个月,而行R1/2切除的患者为11.27个月(P<0.001)。R1/2切除组与未行胃切除术组之间的中位OS时间无差异(P = 0.139)。亚组分析显示,只有接受超过4周期一线化疗的患者从胃切除术中获益(P = 0.018),而接受1 - 4周期一线化疗的患者则未获益(P = 0.275)。多因素分析表明,胃切除术(P = 0.012)和一线化疗周期(P<0.001)是独立的预后因素。胃切除术组的总体术后发病率为3.03%(1/33),未观察到与治疗相关的死亡。本研究表明,姑息化疗后行胃切除术是一种安全的手术,对有腹膜种植的胃癌患者显示出生存获益。此外,临床根治性R0胃切除术和超过4周期的姑息化疗可带来更好的临床结局。