Edinburgh Hypertension Excellence Centre, Clinical Pharmacology Unit, University of Edinburgh, E3.22, QMRI, 47 Little France Crescent, Edinburgh, EH16 4TJ, Scotland, UK.
AbbVie, North Chicago, IL, USA.
Drugs R D. 2017 Sep;17(3):441-448. doi: 10.1007/s40268-017-0201-0.
Fluid retention is a common adverse event in patients who receive endothelin (ET) receptor antagonist therapy, including the highly selective ETA receptor antagonist, atrasentan.
We performed longitudinal assessments of thoracic bioimpedance in patients with type 2 diabetes mellitus and nephropathy to determine whether a decrease in bioimpedance accurately reflected fluid retention during treatment with atrasentan.
We conducted a randomized, double-blind, placebo-controlled study in 48 patients with type 2 diabetes mellitus and nephropathy who were receiving stable doses of renin angiotensin system inhibitors and diuretics.
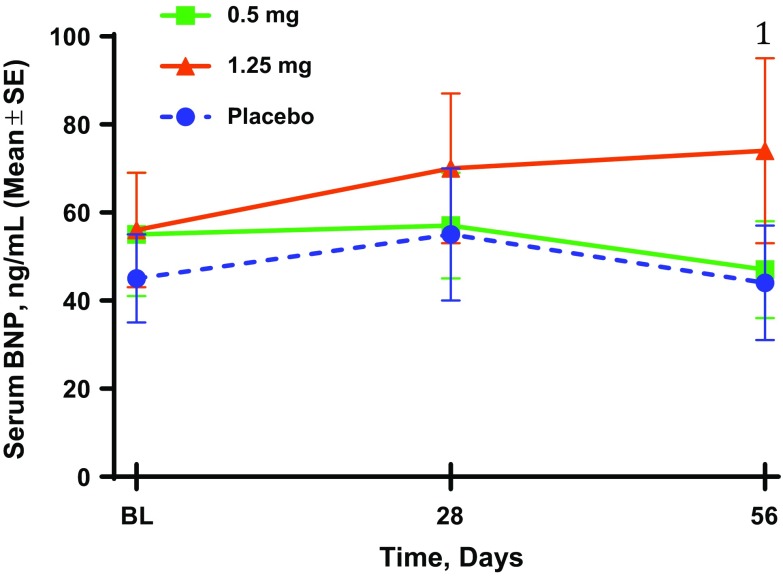
Patients were randomized 1:1:1 to placebo, atrasentan 0.5 mg, or atrasentan 1.25 mg once daily for 8 weeks. Thoracic bioimpedance, vital signs, clinical exams, and serologies were taken at weeks 1, 2, 4, 6, and 8, with the exception of serum hemoglobin, which was not taken at week 1, and serum brain natriuretic peptide, which was only taken at baseline, week 4, and week 8.
Alterations in bioimpedance were more often present in those who received atrasentan than in those who received placebo, though overall differences were not statistically significant. Transient declines in thoracic bioimpedance during the first 2 weeks of atrasentan exposure occurred before or during peak increases in body weight and hemodilution (decreased serum hemoglobin).
We conclude that thoracic bioimpedance did not reflect changes in weight gain or edema with atrasentan treatment in this study. However, the sample size was small, and it may be of interest to explore the use of thoracic bioimpedance in a larger population to understand its potential clinical use in monitoring fluid retention in patients with chronic kidney disease who receive ET receptor antagonists.
流体潴留是接受内皮素(ET)受体拮抗剂治疗的患者的常见不良反应,包括高度选择性的 ETA 受体拮抗剂阿曲生坦。
我们对 2 型糖尿病肾病患者进行了胸部生物阻抗的纵向评估,以确定在接受阿曲生坦治疗期间,生物阻抗的降低是否能准确反映液体潴留。
我们进行了一项随机、双盲、安慰剂对照的研究,纳入了 48 名接受稳定剂量的肾素-血管紧张素系统抑制剂和利尿剂治疗的 2 型糖尿病肾病患者。
患者按照 1:1:1 的比例随机分为安慰剂组、阿曲生坦 0.5mg 组和阿曲生坦 1.25mg 组,每日一次,治疗 8 周。在第 1、2、4、6 和 8 周,测量了胸部生物阻抗、生命体征、临床检查和血清学指标,除了第 1 周不测量血清血红蛋白,第 4 和 8 周只测量基线、第 4 周和第 8 周的血清脑钠肽。
与安慰剂组相比,接受阿曲生坦治疗的患者的生物阻抗改变更常见,尽管总体差异无统计学意义。在阿曲生坦暴露的前 2 周,胸部生物阻抗短暂下降,发生在体重和血液稀释(血清血红蛋白下降)的峰值之前或期间。
我们的结论是,在这项研究中,胸部生物阻抗不能反映阿曲生坦治疗期间体重增加或水肿的变化。然而,样本量较小,探索在更大的人群中使用胸部生物阻抗来了解其在监测接受 ET 受体拮抗剂的慢性肾脏病患者液体潴留方面的潜在临床应用可能会很有趣。