Katikireddi Srinivasa Vittal, Skivington Kathryn, Leyland Alastair H, Hunt Kate, Mercer Stewart W
MRC/CSO Social & Public Health Sciences Unit, University of Glasgow, Top floor, 200 Renfield Street, Glasgow, G2 3QB, United Kingdom.
Department of General Practice & Primary Care, University of Glasgow, 1 Horselethill Road, Glasgow, G12 8UX, Scotland.
BMC Med. 2017 Aug 24;15(1):152. doi: 10.1186/s12916-017-0913-6.
Multimorbidity is a major challenge to health systems globally and disproportionately affects socioeconomically disadvantaged populations. We examined socioeconomic inequalities in developing multimorbidity across the lifecourse and investigated the contribution of five behaviour-related risk factors.
The Twenty-07 study recruited participants aged approximately 15, 35, and 55 years in 1987 and followed them up over 20 years. The primary outcome was development of multimorbidity (2+ health conditions). The relationship between five different risk factors (smoking, alcohol consumption, diet, body mass index (BMI), physical activity) and the development of multimorbidity was assessed. Social patterning in the development of multimorbidity based on two measures of socioeconomic status (area-based deprivation and household income) was then determined, followed by investigation of potential mediation by the five risk factors. Multilevel logistic regression models and predictive margins were used for statistical analyses. Socioeconomic inequalities in multimorbidity were quantified using relative indices of inequality and attenuation assessed through addition of risk factors.
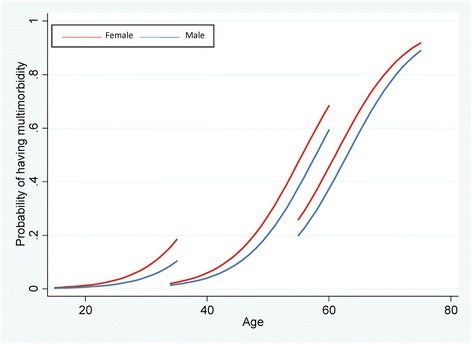
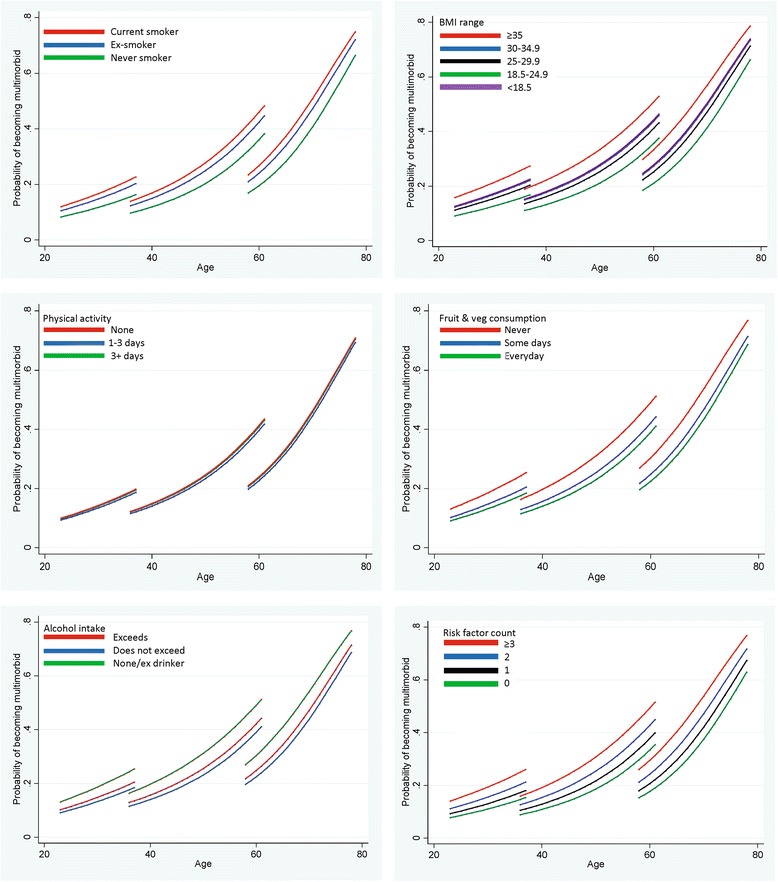
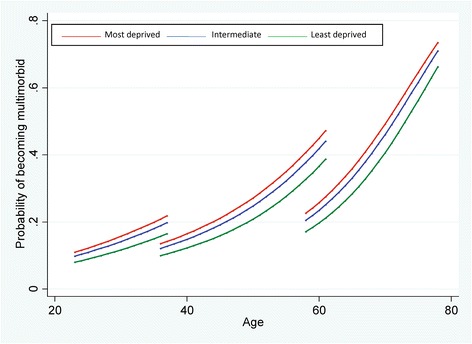
Multimorbidity prevalence increased markedly in all cohorts over the 20 years. Socioeconomic disadvantage was associated with increased risk of developing multimorbidity (most vs least deprived areas: odds ratio (OR) 1.46, 95% confidence interval (CI) 1.26-1.68), and the risk was at least as great when assessed by income (OR 1.53, 95% CI 1.25-1.87) or when defining multimorbidity as 3+ conditions. Smoking (current vs never OR 1.56, 1.36-1.78), diet (no fruit/vegetable consumption in previous week vs consumption every day OR 1.57, 95% CI 1.33-1.84), and BMI (morbidly obese vs healthy weight OR 1.88, 95% CI 1.42-2.49) were strong independent predictors of developing multimorbidity. A dose-response relationship was observed with number of risk factors and subsequent multimorbidity (3+ risk factors vs none OR 1.91, 95% CI 1.57-2.33). However, the five risk factors combined explained only 40.8% of socioeconomic inequalities in multimorbidity development.
Preventive measures addressing known risk factors, particularly obesity and smoking, could reduce the future multimorbidity burden. However, major socioeconomic inequalities in the development of multimorbidity exist even after taking account of known risk factors. Tackling social determinants of health, including holistic health and social care, is necessary if the rising burden of multimorbidity in disadvantaged populations is to be redressed.
多病共存是全球卫生系统面临的一项重大挑战,对社会经济弱势群体的影响尤为严重。我们研究了一生中患多病共存的社会经济不平等现象,并调查了五个与行为相关的风险因素的作用。
“二十 - 07研究”于1987年招募了年龄约为15岁、35岁和55岁的参与者,并对他们进行了20多年的随访。主要结局是多病共存(两种及以上健康状况)的发生情况。评估了五个不同风险因素(吸烟、饮酒、饮食、体重指数(BMI)、身体活动)与多病共存发生之间的关系。然后根据社会经济地位的两种衡量指标(基于地区的贫困程度和家庭收入)确定多病共存发生中的社会模式,随后调查五个风险因素的潜在中介作用。使用多水平逻辑回归模型和预测边际进行统计分析。通过不平等相对指数和添加风险因素评估的衰减来量化多病共存中的社会经济不平等。
在20年期间,所有队列中的多病共存患病率均显著上升。社会经济劣势与患多病共存的风险增加相关(最贫困地区与最不贫困地区相比:优势比(OR)为1.46,95%置信区间(CI)为1.26 - 1.68),按收入评估时风险同样高(OR为1.53,95%CI为1.25 - 1.87),或将多病共存定义为三种及以上状况时也是如此。吸烟(当前吸烟者与从不吸烟者相比,OR为1.56,95%CI为1.36 - 1.78)、饮食(前一周未食用水果/蔬菜与每天食用相比,OR为1.57,95%CI为1.33 - 1.84)和BMI(病态肥胖与健康体重相比,OR为1.88,95%CI为1.42 - 2.49)是患多病共存的强有力独立预测因素。观察到风险因素数量与随后的多病共存之间存在剂量反应关系(三个及以上风险因素与无风险因素相比,OR为1.91,95%CI为1.57 - 2.33)。然而,五个风险因素综合起来仅解释了多病共存发生中社会经济不平等的40.8%。
针对已知风险因素,特别是肥胖和吸烟的预防措施,可减轻未来的多病共存负担。然而,即使考虑了已知风险因素,在多病共存的发生方面仍存在重大的社会经济不平等。如果要纠正弱势群体中不断上升的多病共存负担,就必须解决健康的社会决定因素,包括全面的健康和社会护理。