Gurung Santosh, Harris Jennifer B, Eltayeb Abu Obeida, Hampton Lee M, Diorditsa Sergey, Avagyan Tigran, Schluter W William
World Health Organization Western Pacific Regional Office, Manila, Philippines.
Global Immunization Division, Centers for Disease Control and Prevention, Atlanta Georgia.
J Infect Dis. 2017 Jul 1;216(suppl_1):S101-S108. doi: 10.1093/infdis/jiw574.
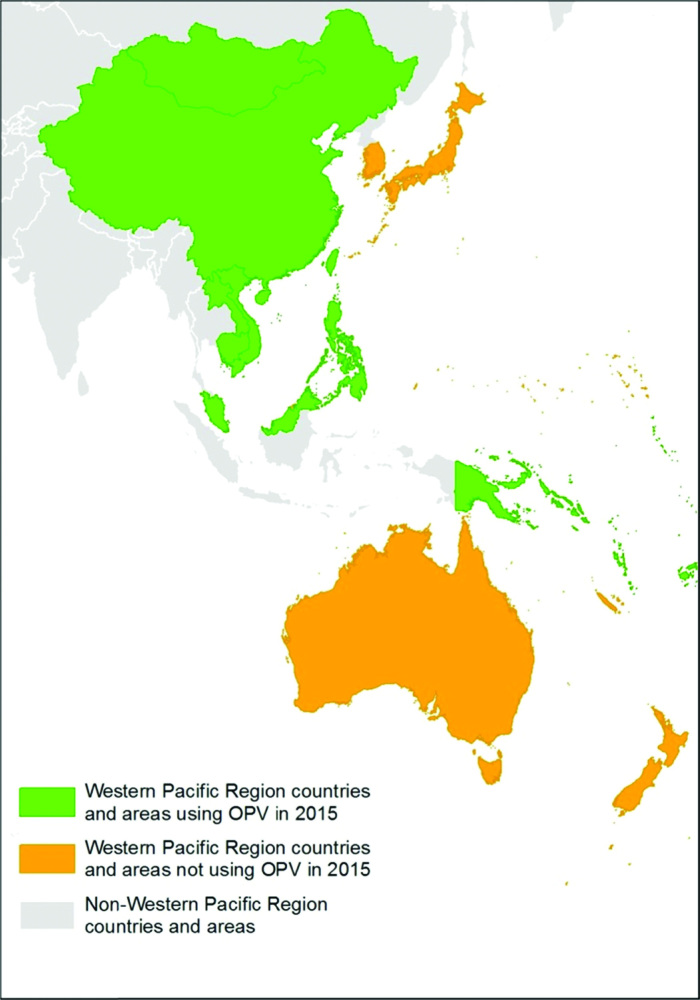
The World Health Organization (WHO) Western Pacific Region (WPR) has maintained its polio-free status since 2000. The emergence of vaccine-derived polioviruses (VDPVs), however, remains a risk, as oral polio vaccine (OPV) is still used in many of the region's countries, and pockets of unimmunized or underimmunized children exist in some countries. From 2014 to 2016, the region participated in the globally coordinated efforts to introduce inactivated polio vaccine (IPV) into all countries that did not yet include it in their national immunization schedules, and to "switch" from trivalent OPV (tOPV) to bivalent OPV (bOPV) in all countries still using OPV in 2016.As of September 2016, 15 of 17 countries and areas that did not use IPV by the end of 2014 had introduced IPV. Introduction in the remaining 2 countries has been delayed because of the global shortage of IPV, making it unavailable to select lower-risk countries until the fourth quarter of 2017. All 16 countries using OPV as of 2016 successfully withdrew tOPV during the globally synchronized switch from April to May 2016, and 15 of 16 countries introduced bOPV at the same time, with the remaining country introducing it within 30 days. While countries were primarily responsible for self-funding these activities, additional support was provided.The main challenges encountered in the Western Pacific Region with both IPV introduction and the tOPV-bOPV switch were related to overcoming regulatory policies and challenges with vaccine procurement. As a result, substantial lead time was needed to resolve procurement and regulatory issues before the introductions of IPV and bOPV. As the global community prepares for the full removal of all OPV from immunization programs, this need for lead time and consideration of the impact on national policies should be considered.
自2000年以来,世界卫生组织(WHO)西太平洋区域(WPR)一直保持无脊髓灰质炎状态。然而,疫苗衍生脊髓灰质炎病毒(VDPV)的出现仍然是一个风险,因为该区域许多国家仍在使用口服脊髓灰质炎疫苗(OPV),而且一些国家存在未免疫或免疫不足的儿童群体。2014年至2016年,该区域参与了全球协调的努力,将灭活脊髓灰质炎疫苗(IPV)引入所有尚未将其纳入国家免疫规划的国家,并在2016年仍在使用OPV的所有国家从三价OPV(tOPV)“转换”为二价OPV(bOPV)。截至2016年9月,2014年底未使用IPV的17个国家和地区中有15个已引入IPV。其余2个国家的引入工作因IPV全球短缺而推迟,直到2017年第四季度才可供风险较低的国家选用。截至2016年使用OPV的所有16个国家在2016年4月至5月的全球同步转换期间成功停用了tOPV,16个国家中有15个同时引入了bOPV,其余国家在30天内引入。虽然各国主要负责为这些活动自筹资金,但也提供了额外支持。西太平洋区域在引入IPV和tOPV - bOPV转换过程中遇到的主要挑战与克服监管政策以及疫苗采购方面的挑战有关。因此,在引入IPV和bOPV之前,需要大量准备时间来解决采购和监管问题。随着国际社会为全面从免疫规划中停用所有OPV做准备,应考虑到这种对准备时间的需求以及对国家政策的影响。