Trivin Claire, Tran Antoine, Moulin Bruno, Choukroun Gabriel, Gatault Philippe, Courivaud Cécile, Augusto Jean-François, Ficheux Maxence, Vigneau Cécile, Thervet Eric, Karras Alexandre
Department of Nephrology, Hopital Europeen Georges Pompidou, Paris, France.
Pediatric Emergency, Hopitaux pediatrique CHU Nice Lenval, France.
Clin Kidney J. 2017 Aug;10(4):461-469. doi: 10.1093/ckj/sfw101. Epub 2016 Nov 10.
Recent years have seen increasing use of rituximab (RTX) for various types of primary and secondary glomerulopathies. However, there are no studies that specifically address the risk of infection related to this agent in patients with these conditions.
We reviewed the outcomes of all patients who received RTX therapy for glomerular disease between June 2000 and October 2011 in eight French nephrology departments. Each case was analysed for survival, cause of death if a non-survivor and/or the presence of infectious complications, including severe or opportunistic infection occurring within the 12 months following RTX infusion.
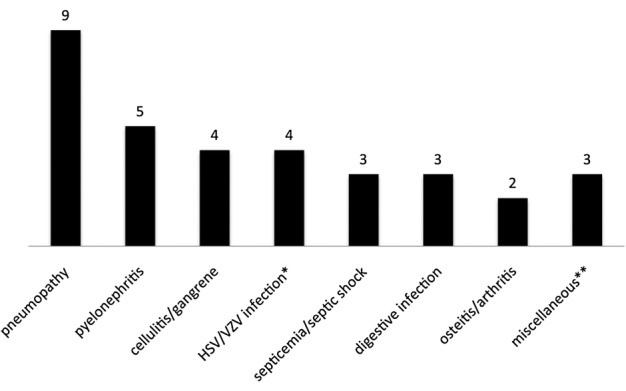
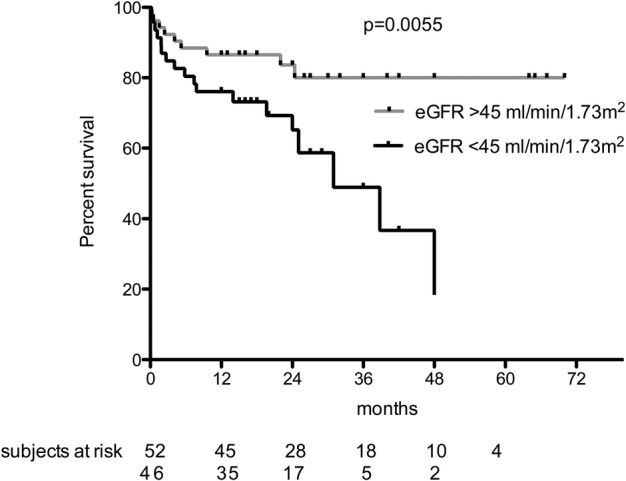
Among 98 patients treated with RTX, 25 presented with at least one infection. We report an infection rate of 21.6 per 100 patient-years. Five patients died within 12 months following an RTX infusion, of whom four also presented with an infection. The median interval between the last RTX infusion and the first infectious episode was 2.1 months (interquartile range 0.5-5.1). Most infections were bacterial (79%) and pneumonia was the most frequent infection reported (27%). The presence of diabetes mellitus (P = 0.006), the cumulative RTX dose (P = 0.01) and the concomitant use of azathioprine (P = 0.03) were identified as independent risk factors. Renal failure was significantly associated with an increased infection risk by bivariate analysis (P = 0.03) and was almost significant by multivariate analysis (P = 0.05). Nephrotic syndrome did not further increase the risk of infection and/or death.
The risk of infection after RTX-based immunosuppression among patients with glomerulopathy must be considered and patients should receive close monitoring and appropriate infection prophylaxis, especially in those with diabetes and high-dose RTX regimens.
近年来,利妥昔单抗(RTX)在各类原发性和继发性肾小球疾病中的应用日益增多。然而,尚无专门针对患有这些疾病的患者使用该药物相关感染风险的研究。
我们回顾了2000年6月至2011年10月期间在法国八个肾脏病科接受RTX治疗肾小球疾病的所有患者的治疗结果。分析每个病例的生存情况、非幸存者的死亡原因和/或感染并发症的存在情况,包括RTX输注后12个月内发生的严重或机会性感染。
在98例接受RTX治疗的患者中,25例出现至少一次感染。我们报告的感染率为每100患者年21.6例。5例患者在RTX输注后12个月内死亡,其中4例也出现了感染。最后一次RTX输注与首次感染发作之间的中位间隔为2.1个月(四分位间距0.5 - 5.1)。大多数感染为细菌感染(79%),报告最多的感染是肺炎(27%)。糖尿病的存在(P = 0.006)、RTX累积剂量(P = 0.01)和硫唑嘌呤的联合使用(P = 0.03)被确定为独立危险因素。通过双变量分析,肾衰竭与感染风险增加显著相关(P = 0.03),通过多变量分析几乎具有显著性(P = 0.05)。肾病综合征并未进一步增加感染和/或死亡风险。
必须考虑肾小球病患者基于RTX的免疫抑制治疗后的感染风险,患者应接受密切监测和适当的感染预防,尤其是糖尿病患者和接受高剂量RTX治疗方案的患者。