Litchfield Ian J, Bentham Louise M, Lilford Richard J, McManus Richard J, Hill Ann, Greenfield Sheila
Institute of Applied Health Research, College of Medical and Dental Sciences, University of Birmingham, Edgbaston, Birmingham, B15 2TT, UK.
WMS - Population Evidence and Technologies, University of Warwick, Coventry, UK.
BMC Health Serv Res. 2017 Aug 30;17(1):615. doi: 10.1186/s12913-017-2566-8.
Increasing numbers of blood tests are being ordered in primary care settings and the swift and accurate communication of test results is central to providing high quality care. The process of testing and result communication is complex and reliant on the coordinated actions of care providers, external groups in laboratory and hospital settings, and patients. This fragmentation leaves it vulnerable to error and the need to improve an apparently fallible system is apparent. However, primary care is complex and does not necessarily adopt change in a linear and prescribed manner influenced by a range of factors relating to practice staff, patients and organisational factors. To account for these competing perspectives, we worked in conjunction with both staff and patients to develop and implement strategies intended to improve patient satisfaction and increase efficiency of existing processes.
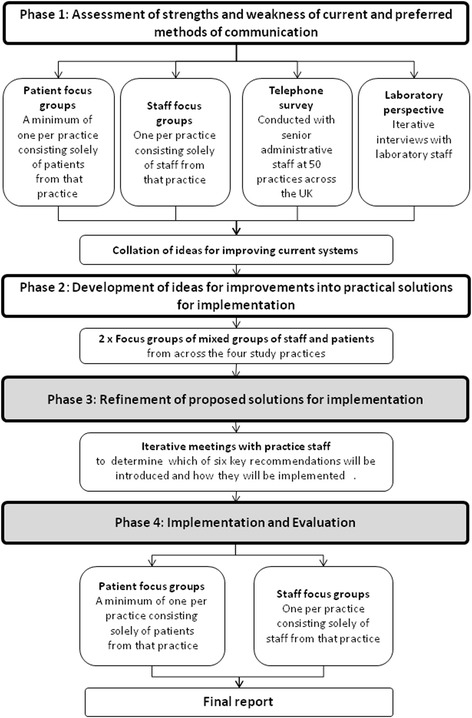
The study applied the principles of 'experience-based co-design' to identify key areas of weakness and source proposals for change from staff and patients. The study was undertaken within two primary practices situated in South Birmingham (UK) of contrasting size and socio-economic environment. Senior practice staff were involved in the refinement of the interventions for introduction. We conducted focus groups singly constituted of staff and patients at each practice to determine suitability, applicability and desirability alongside the practical implications of their introduction.
At each practice four of the six proposals for change were implemented these were increased access to phlebotomy, improved receptionist training, proactive communication of results, and increased patient awareness of the tests ordered and the means of their communication. All were received favourably by both patients and staff. The remaining issues around the management of telephone calls and the introduction of electronic alerts for missing results were not addressed due to constraints of time and available resources.
Approaches to tackling the same area of weakness differed at practices and was determined by individual staff attitudes and by organisational and patient characteristics. The long-term impact of the changes requires further quantitative evaluation.
基层医疗环境中要求进行的血液检测数量日益增加,检测结果的迅速准确传达是提供高质量医疗服务的核心。检测及结果传达过程复杂,依赖于医疗服务提供者、实验室和医院环境中的外部团体以及患者的协同行动。这种分散性使其容易出错,显然需要改进这个看似易出故障的系统。然而,基层医疗情况复杂,不一定会以线性且规定好的方式接受变革,这受到一系列与执业人员、患者及组织因素相关的影响。为了兼顾这些相互矛盾的观点,我们与工作人员和患者合作,制定并实施旨在提高患者满意度和提升现有流程效率的策略。
该研究应用“基于体验的协同设计”原则,以确定薄弱环节的关键领域,并从工作人员和患者那里获取变革建议。研究在英国伯明翰南部两个规模和社会经济环境不同的基层医疗机构中进行。资深执业人员参与了引入干预措施的优化工作。我们在每个医疗机构分别组织了由工作人员和患者组成的焦点小组,以确定这些措施的适用性、可行性和可取性以及引入后的实际影响。
在每个医疗机构,六项变革建议中有四项得以实施,即增加静脉穿刺服务的可及性、改进接待员培训、主动传达检测结果,以及提高患者对所开检测项目及其传达方式的认知。患者和工作人员对所有这些措施都给予了好评。由于时间和可用资源的限制,有关电话管理和引入结果缺失电子警报的其余问题未得到解决。
不同医疗机构处理同一薄弱环节的方法不同,这取决于工作人员的个人态度以及组织和患者的特点。这些变革的长期影响需要进一步进行定量评估。