Empen Klaus, Hummel Astrid, Beug Daniel, Felix Stephan B, Busch Mathias C, Kaczmarek Piotr M
Medizinische Klinik B, Universitätsmedizin Greifswald, Sauerbruchstrasse, 17475, Greifswald, Germany.
BMC Res Notes. 2017 Jul 25;10(1):311. doi: 10.1186/s13104-017-2628-3.
Vasculitides are commonly unrecognized causes of coronary stenosis and myocardial ischemia. We report on a 24-year old patient with Takayasu's arteritis who underwent urgent percutaneous coronary intervention, suffered from symptomatic restenosis of the left main coronary artery during standard immunosuppressive therapy.
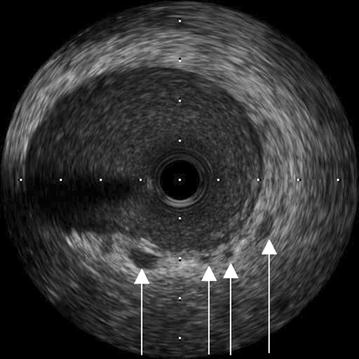
A 24-year old woman was referred for coronary angiography because of typical progressive angina pectoris. On bicycle ergometry, there were both reproducible symptoms and deep ST segment depressions on precordial leads. Semi-selective angiography of the left coronary artery revealed high-grade ostial stenosis. Because of persistent angina pectoris and electrocardiographic signs of acute myocardial ischemia, immediate percutaneous coronary angioplasty with subsequent implantation of an everolimus-eluting stent was performed. This intervention was performed with excellent angiographic results. Because of several concomitant criteria including hypoechogenicity on postprocedural intravascular ultrasonography, the diagnosis of Takayasu's disease was made. The patient was treated with prednisolone and cyclophosphamide for 5 months. Because of recurrent angina pectoris, another coronary angiography was performed, which revealed high-grade in-stent-restenosis. Immunomodulatory therapy was switched to high-dose prednisolone and the anti-IL-6 receptor antagonist tocilizumab. The high-grade in-stent-restenosis persisted, and aortocoronary bypass graft surgery was performed with two saphenous vein grafts to the left anterior descending and circumflex artery. Since then, the patient has been doing well for 2 years.
In cases of treatment refractoriness during standard immunosuppressive therapy, more recently developed biological compounds may offer an alternative strategy.
血管炎是冠状动脉狭窄和心肌缺血常见的未被认识的病因。我们报告一例24岁的Takayasu动脉炎患者,该患者接受了紧急经皮冠状动脉介入治疗,在标准免疫抑制治疗期间左主干冠状动脉出现有症状的再狭窄。
一名24岁女性因典型的进行性心绞痛被转诊进行冠状动脉造影。在自行车运动试验中,出现了可重复的症状,胸前导联有深ST段压低。左冠状动脉半选择性血管造影显示高位开口狭窄。由于持续的心绞痛和急性心肌缺血的心电图表现,立即进行了经皮冠状动脉血管成形术并随后植入依维莫司洗脱支架。该干预取得了良好的血管造影结果。由于包括术后血管内超声检查显示低回声在内的几个伴随标准,确诊为Takayasu病。患者接受泼尼松龙和环磷酰胺治疗5个月。由于复发性心绞痛,再次进行冠状动脉造影,显示支架内高度再狭窄。免疫调节治疗改为大剂量泼尼松龙和抗IL-6受体拮抗剂托珠单抗。支架内高度再狭窄持续存在,遂进行主动脉冠状动脉搭桥手术,用两根大隐静脉移植至左前降支和回旋支动脉。从那时起,患者两年来情况良好。
在标准免疫抑制治疗期间出现治疗难治性的病例中,最近开发的生物化合物可能提供一种替代策略。