Fernandes Dália, Domingues Sara, Gonçalves Bruno Moreira, Bastos Pedro, Ferreira Aníbal, Rodrigues António, Gonçalves Raquel, Lopes Luís, Rolanda Carla
Gastroenterology Department, Hospital de Braga, Braga, Portugal.
GE Port J Gastroenterol. 2016 Jan 29;23(2):66-75. doi: 10.1016/j.jpge.2015.10.005. eCollection 2016 Mar-Apr.
Colorectal cancer presents itself as acute bowel occlusion in 10-40% of patients. There are two main therapeutic approaches: urgent surgery and endoluminal placement self-expandable metallic stents (SEMS).
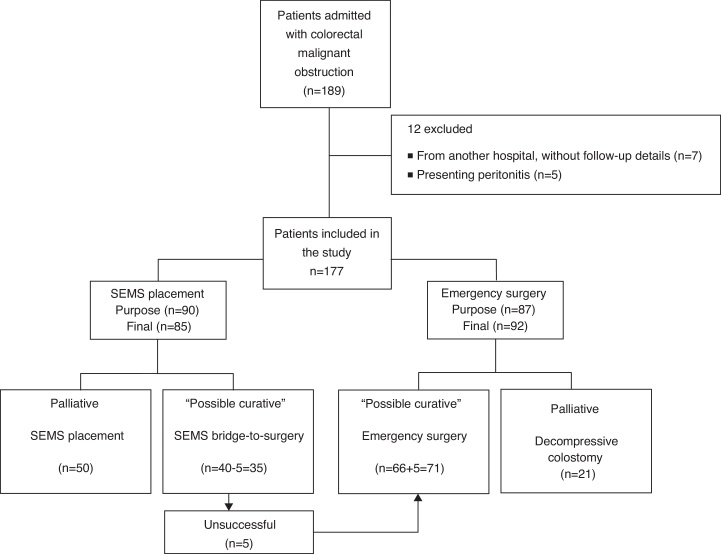
This study intended to better clarify the risk/benefit ratio of the above-mentioned approaches. We conducted a retrospective longitudinal multicenter study, including 189 patients with acute malignant colorectal occlusion, diagnosed between January 2005 and March 2013.
Globally (85 patients - 35 bridge-to-surgery and 50 palliative), SEMS's technical success was of 94%. Palliative SEMS had limited clinical success (60%) and were associated with 40% of complications. SEMS occlusion (19%) was the most frequent complication, followed by migration (9%) and bowel perforation (7%). Elective surgery after stenting was associated with a higher frequency of primary anastomosis (94% vs. 76%; = 0.038), and a lower rate of colostomy (26% vs. 55%; = 0.004) and overall mortality (31% vs. 57%; = 0.02). However, no significant differences were identified concerning postoperative complications. Regarding palliative treatment, no difference was found in the complications rate and overall mortality between SEMS and decompressive colostomy/ileostomy. In this SEMS subgroup, we found a higher rate of reinterventions (40% vs. 5%; = 0.004) and a longer hospital stay (14, nine vs. seven, three days; = 0.004).
SEMS placement as a bridge-to-surgery should be considered in the acute treatment of colorectal malignant occlusion, since it displays advantages regarding primary anastomosis, colostomy rate and overall mortality. In contrast, in this study, palliative SEMS did not appear to present significant advantages when compared to decompressive colostomy.
10% - 40%的结直肠癌患者表现为急性肠梗阻。主要有两种治疗方法:急诊手术和腔内放置自膨式金属支架(SEMS)。
本研究旨在更好地阐明上述方法的风险/效益比。我们进行了一项回顾性纵向多中心研究,纳入了2005年1月至2013年3月期间诊断为急性恶性结直肠梗阻的189例患者。
总体而言(85例患者 - 35例作为手术过渡和50例姑息治疗),SEMS的技术成功率为94%。姑息性SEMS的临床成功率有限(60%),且并发症发生率为40%。SEMS堵塞(19%)是最常见的并发症,其次是移位(9%)和肠穿孔(7%)。支架置入后的择期手术与更高的一期吻合率(94%对76%;P = 0.038)、更低的结肠造口率(26%对55%;P = 0.004)和更低的总体死亡率(31%对57%;P = 0.02)相关。然而,术后并发症方面未发现显著差异。关于姑息治疗,SEMS与减压结肠造口术/回肠造口术在并发症发生率和总体死亡率方面未发现差异。在这个SEMS亚组中,我们发现再次干预率更高(40%对5%;P = 0.004)且住院时间更长(14.9天对7.3天;P = 0.004)。
在结直肠恶性梗阻的急性治疗中,应考虑将SEMS置入作为手术过渡,因为它在一期吻合、结肠造口率和总体死亡率方面具有优势。相比之下,在本研究中,与减压结肠造口术相比,姑息性SEMS似乎没有明显优势。