Farrell Maureen, Yoneda Zachary, Montgomery Jay, Crawford Diane, Wray Lauren Lee, Xu Meng, Kolek Matthew J, Richardson Travis, Lugo Ricardo, Metawee Mohamed, Michaud Greg, Estrada Juan Carlos, Saavedra Pablo, Shen Sharon, Kanagasundram Arvindh, Ellis Christopher R, Crossley George, Roden Dan, Shoemaker M Benjamin
Department of Medicine, Vanderbilt University Medical Center, Nashville, Tennessee, United States of America.
Department of Biostatistics, Vanderbilt University, Nashville, Tennessee, United States of America.
PLoS One. 2017 Sep 7;12(9):e0184354. doi: 10.1371/journal.pone.0184354. eCollection 2017.
Atrial fibrillation (AF) is a mechanistically heterogeneous disorder, and the ability to identify sub-phenotypes ("endophenotypes") of AF would assist in the delivery of personalized medicine. We used the clinical response to pulmonary vein isolation (PVI) to identify a sub-group of patients with non-PV mediated AF and sought to define the clinical associations.
Subjects enrolled in the Vanderbilt AF Ablation Registry who underwent a repeat AF ablation due to arrhythmia recurrence were analyzed on the basis of PV reconnection. Subjects who had no PV reconnection were defined as "non-PV mediated AF". A comparison group of subjects were identified who had AF that was treated with PVI-only and experienced no arrhythmia recurrence >12 months. They were considered a group enriched for "PV-mediated AF". Univariate and multivariable binary logistic regression analysis was performed to investigate clinical associations between the PV and non-PV mediated AF groups.
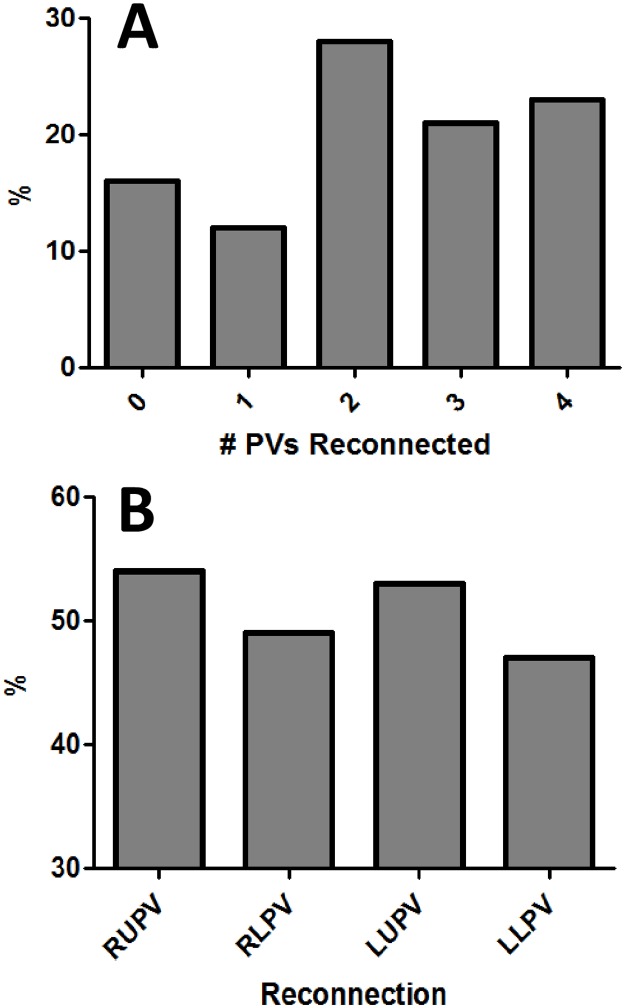
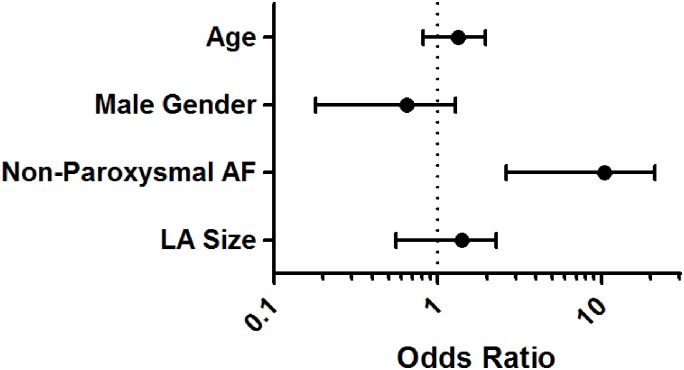
Two hundred and twenty nine subjects underwent repeat AF ablation and thirty three (14%) had no PV reconnection. They were compared with 91 subjects identified as having PV-mediated AF. Subjects with non-PV mediated AF were older (64 years [IQR 60,71] vs. 60 [52,67], P = 0.01), more likely to have non-paroxysmal AF (82% [N = 27] vs. 35% [N = 32], P<0.001), and had a larger left atrium (LA) (4.2cm [3.6,4.8] vs. 4.0 [3.3,4.4], P = 0.04). In univariate analysis, age (per decade: OR 1.56 [95% CI: 1.04 to 2.33], P = 0.03), LA size (per cm: OR 1.8 [1.06 to 3.21], P = 0.03) and non-paroxysmal AF (OR 8.3 [3.10 to 22.19], P<0.001) were all significantly associated with non-PV mediated AF. However, in multivariable analysis only non-paroxysmal AF was independently associated with non-PV mediated AF (OR 7.47 [95% CI 2.62 to 21.29], P<0.001), when adjusted for age (per decade: OR 1.25 [0.81 to 1.94], P = 0.31), male gender (OR 0.48 [0.18 to 1.28], P = 0.14), and LA size (per 1cm: 1.24 [0.65 to 2.33], P = 0.52).
Non-paroxysmal AF was the only clinical variable found to be independently associated with non-PV mediated AF. We demonstrated that analysis of AF ablation outcomes data can serve as a tool to successfully identify a sub-phenotype of subjects who have non-PV mediated AF.
ClinicalTrials.gov ID # NCT02404415.
心房颤动(AF)是一种机制异质性疾病,识别AF的亚表型(“内表型”)有助于实现个性化医疗。我们利用肺静脉隔离(PVI)的临床反应来识别非肺静脉介导的AF患者亚组,并试图确定其临床关联。
对范德比尔特AF消融登记处中因心律失常复发而接受重复AF消融的受试者,根据肺静脉重新连接情况进行分析。无肺静脉重新连接的受试者被定义为“非肺静脉介导的AF”。确定一组仅接受PVI治疗且12个月以上无心律失常复发的AF受试者作为对照组。他们被视为富含“肺静脉介导的AF”的组。进行单变量和多变量二元逻辑回归分析,以研究肺静脉介导和非肺静脉介导的AF组之间的临床关联。
229名受试者接受了重复AF消融,33名(14%)无肺静脉重新连接。将他们与91名被确定为有肺静脉介导的AF的受试者进行比较。非肺静脉介导的AF受试者年龄更大(64岁[四分位间距60,71]对60[52,67],P = 0.01),更可能有非阵发性AF(82%[N = 27]对35%[N = 32],P<0.001),左心房(LA)更大(4.2cm[3.6,4.8]对4.0[3.3,4.4],P = 0.04)。在单变量分析中,年龄(每十年:比值比1.56[95%置信区间:1.04至2.33],P = 0.03)、LA大小(每厘米:比值比1.8[1.06至3.21],P = 0.03)和非阵发性AF(比值比8.3[3.10至22.19],P<0.001)均与非肺静脉介导的AF显著相关。然而,在多变量分析中,调整年龄(每十年:比值比1.25[0.81至1.94],P = 0.31)、男性性别(比值比0.48[0.18至1.28],P = 0.14)和LA大小(每1cm:1.24[0.65至2.33],P = 0.52)后,仅非阵发性AF与非肺静脉介导的AF独立相关(比值比7.47[95%置信区间2.62至21.29],P<0.001)。
非阵发性AF是唯一被发现与非肺静脉介导的AF独立相关的临床变量。我们证明,对AF消融结果数据的分析可作为一种工具,成功识别非肺静脉介导的AF受试者的亚表型。
ClinicalTrials.gov标识符#NCT02404415。