Unruh Mark L, Pankratz V Shane, Demko John E, Ray Evan C, Hughey Rebecca P, Kleyman Thomas R
Nephrology Division, Department of Internal Medicine, University of New Mexico, Albuquerque NM.
New Mexico VA Health Care System, Albuquerque, NM.
Kidney Int Rep. 2017 Sep;2(5):893-904. doi: 10.1016/j.ekir.2017.05.008. Epub 2017 May 17.
Renal Na retention and extracellular fluid volume expansion are hallmarks of nephrotic syndrome, which occurs even in the absence of activation of hormones that stimulate renal Na transporters. Plasmin-dependent activation of the epithelial Na channel (ENaC) has been proposed to have a role in renal Na retention in the setting of nephrotic syndrome. We hypothesized that the ENaC inhibitor amiloride would be an effective therapeutic agent in inducing a natriuresis and lowering blood pressure in individuals with macroscopic proteinuria.
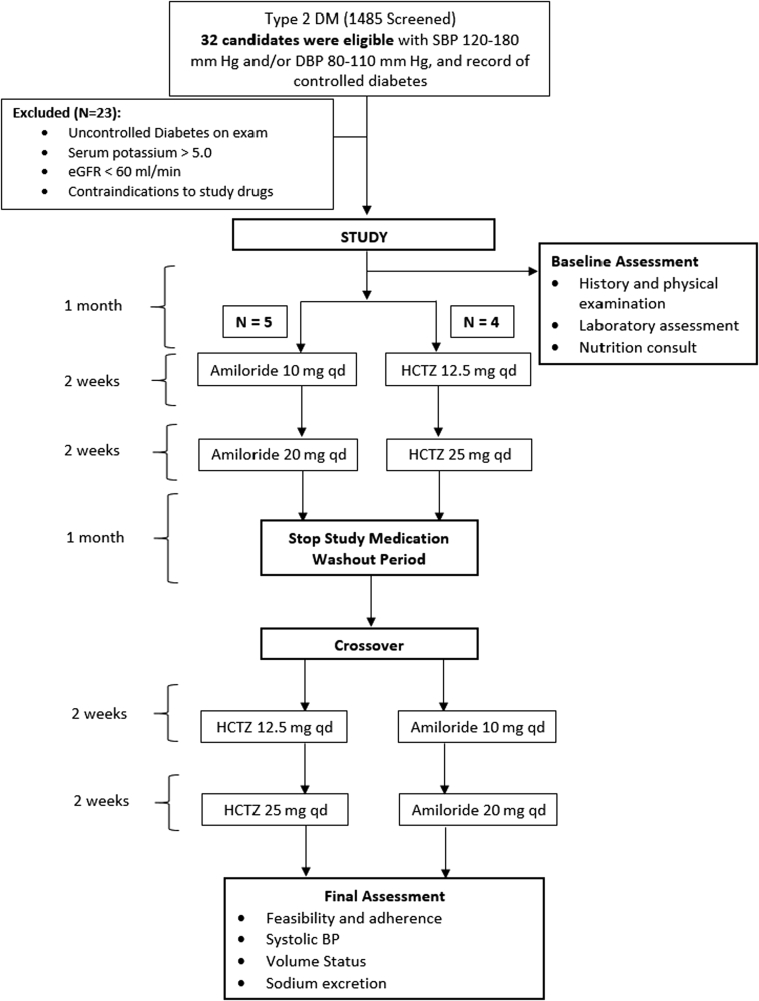
We conducted a pilot double-blind randomized cross-over study comparing the effects of daily administration of either oral amiloride or hydrochlorothiazide (HCTZ) to patients with type 2 diabetes and macroscopic proteinuria. Safety and efficacy were assessed by monitoring systolic blood pressure (SBP), kidney function, adherence, weight, urinary Na excretion and serum electrolytes. Nine subjects were enrolled in the trial.
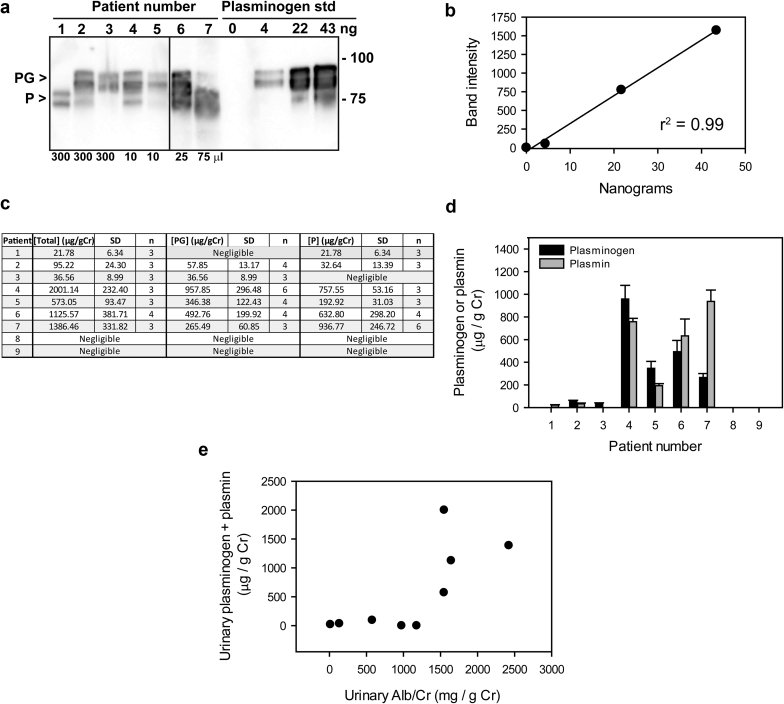
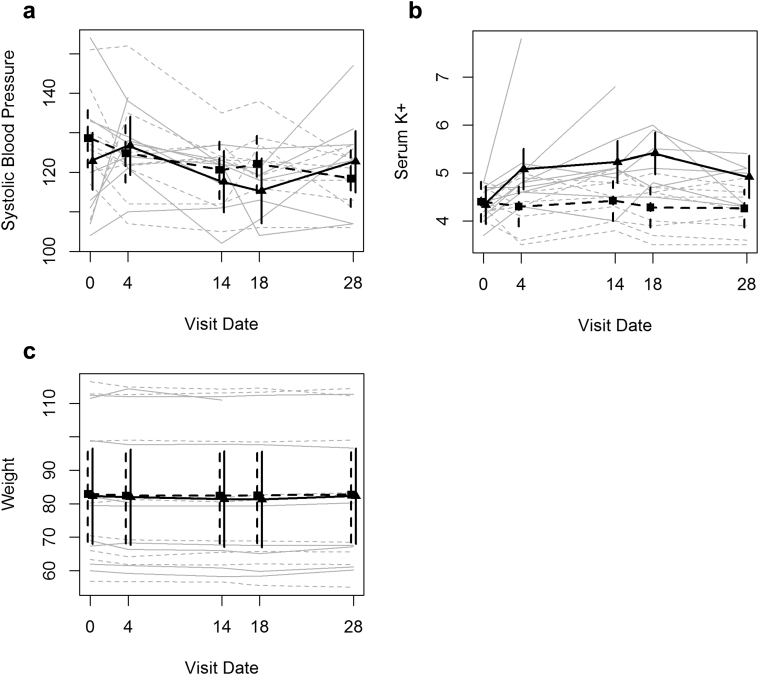
No significant difference in SBP or weight was seen between HCTZ and amiloride (p≥0.15). Amiloride induced differences in serum K (p<0.001), with a 0.88±0.30 mmol/L greater acute increase observed. Two subjects developed acute kidney injury and hyperkalemia when treated with amiloride. Four subjects had readily detectable levels of urinary plasminogen plus plasmin (uPl), and five did not. Changes in SBP in response to amiloride did not differ between individuals with vs. those without detectable uPl.
In summary, among patients with type 2 diabetes, normal renal function and proteinuria, there were reductions in SBP in groups treated with HCTZ or amiloride. Acute kidney injury and severe hyperkalemia were safety concerns with amiloride.
肾钠潴留和细胞外液量增加是肾病综合征的特征,即使在刺激肾钠转运体的激素未激活的情况下也会发生。有人提出,纤溶酶依赖性上皮钠通道(ENaC)激活在肾病综合征时的肾钠潴留中起作用。我们假设,ENaC抑制剂阿米洛利将是诱导大量蛋白尿患者产生利钠作用并降低血压的有效治疗药物。
我们进行了一项初步双盲随机交叉研究,比较每日口服阿米洛利或氢氯噻嗪(HCTZ)对2型糖尿病和大量蛋白尿患者的影响。通过监测收缩压(SBP)、肾功能、依从性、体重、尿钠排泄和血清电解质来评估安全性和疗效。9名受试者参与了该试验。
HCTZ和阿米洛利之间在SBP或体重方面无显著差异(p≥0.15)。阿米洛利引起血清钾差异(p<0.001),观察到急性升高幅度大0.88±0.30 mmol/L。两名受试者在接受阿米洛利治疗时发生急性肾损伤和高钾血症。4名受试者尿纤溶酶原加纤溶酶(uPl)水平易于检测到,5名则未检测到。有或没有可检测到uPl的个体对阿米洛利反应的SBP变化无差异。
总之,在2型糖尿病、肾功能正常和蛋白尿患者中,HCTZ或阿米洛利治疗组的SBP均有所降低。急性肾损伤和严重高钾血症是阿米洛利的安全性问题。