Clark Andrew, Black Robert, Tate Jacqueline, Roose Anna, Kotloff Karen, Lam Diana, Blackwelder William, Parashar Umesh, Lanata Claudio, Kang Gagandeep, Troeger Christopher, Platts-Mills James, Mokdad Ali, Sanderson Colin, Lamberti Laura, Levine Myron, Santosham Mathuram, Steele Duncan
London School of Hygiene and Tropical Medicine, London, United Kingdom.
Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, United States of America.
PLoS One. 2017 Sep 11;12(9):e0183392. doi: 10.1371/journal.pone.0183392. eCollection 2017.
Rotavirus is a leading cause of diarrhoeal mortality in children but there is considerable disagreement about how many deaths occur each year.
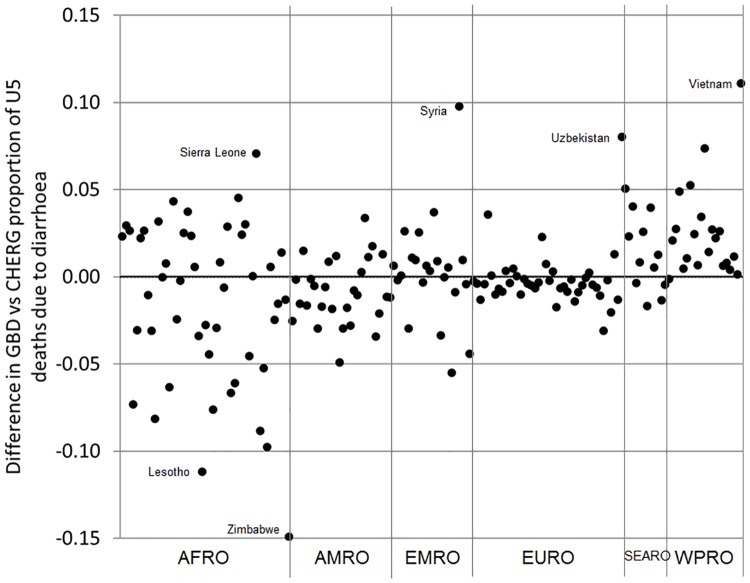
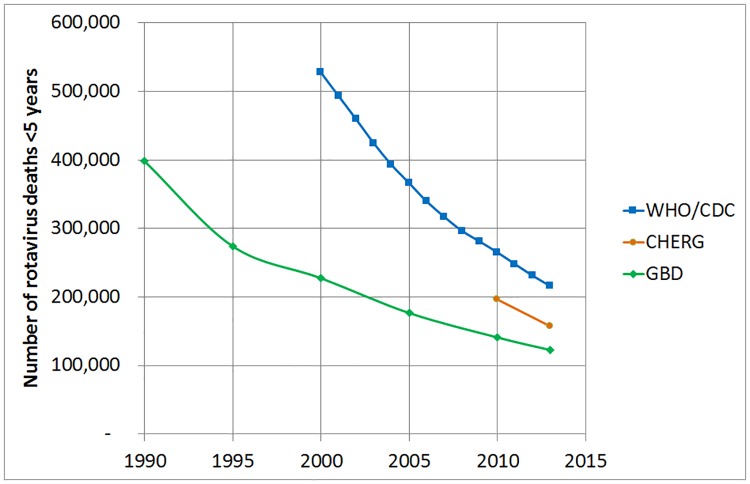
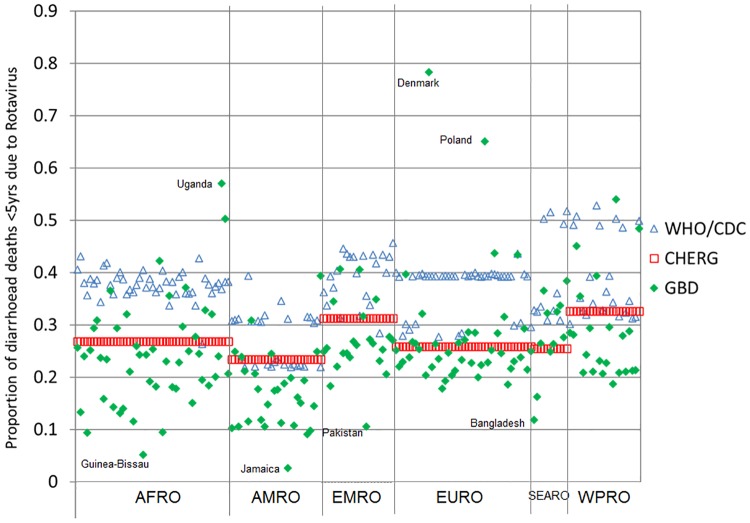
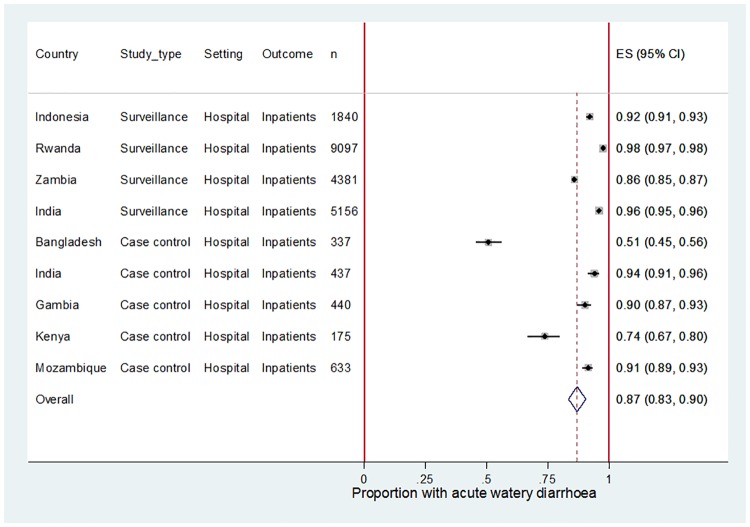
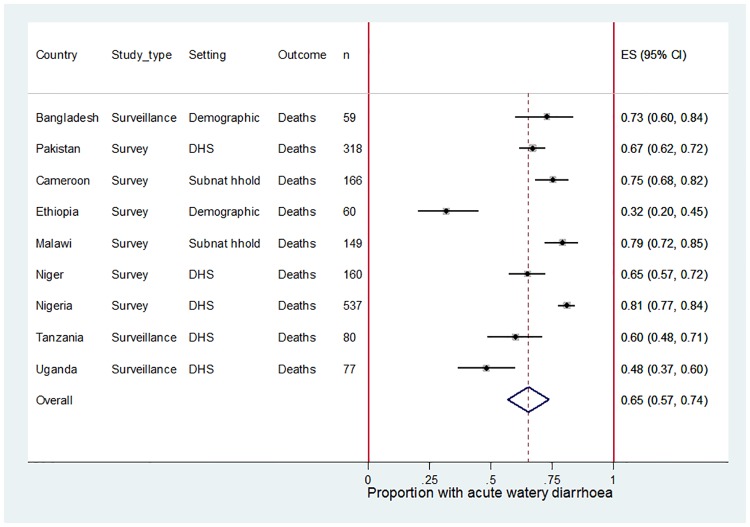
We compared CHERG, GBD and WHO/CDC estimates of age under 5 years (U5) rotavirus deaths at the global, regional and national level using a standard year (2013) and standard list of 186 countries. The global estimates were 157,398 (CHERG), 122,322 (GBD) and 215,757 (WHO/CDC). The three groups used different methods: (i) to select data points for rotavirus-positive proportions; (ii) to extrapolate data points to individual countries; (iii) to account for rotavirus vaccine coverage; (iv) to convert rotavirus-positive proportions to rotavirus attributable fractions; and (v) to calculate uncertainty ranges. We conducted new analyses to inform future estimates. We found that acute watery diarrhoea was associated with 87% (95% CI 83-90%) of U5 diarrhoea hospitalisations based on data from 84 hospital sites in 9 countries, and 65% (95% CI 57-74%) of U5 diarrhoea deaths based on verbal autopsy reports from 9 country sites. We reanalysed data from the Global Enteric Multicenter Study (GEMS) and found 44% (55% in Asia, and 32% in Africa) rotavirus-positivity among U5 acute watery diarrhoea hospitalisations, and 28% rotavirus-positivity among U5 acute watery diarrhoea deaths. 97% (95% CI 95-98%) of the U5 diarrhoea hospitalisations that tested positive for rotavirus were entirely attributable to rotavirus. For all clinical syndromes combined the rotavirus attributable fraction was 34% (95% CI 31-36%). This increased by a factor of 1.08 (95% CI 1.02-1.14) when the GEMS results were reanalysed using a more sensitive molecular test.
We developed consensus on seven proposals for improving the quality and transparency of future rotavirus mortality estimates.
轮状病毒是导致儿童腹泻死亡的主要原因,但对于每年有多少儿童死于轮状病毒感染,各方存在很大分歧。
我们使用标准年份(2013年)和186个国家的标准列表,比较了儿童健康流行病学参考小组(CHERG)、全球疾病负担研究(GBD)以及世界卫生组织/美国疾病控制与预防中心(WHO/CDC)对全球、区域和国家层面5岁以下儿童轮状病毒死亡人数的估计。全球层面的估计数字分别为:157,398例(CHERG)、122,322例(GBD)和215,757例(WHO/CDC)。这三个组织采用了不同的方法:(i)选择轮状病毒阳性比例的数据点;(ii)将数据点外推至各个国家;(iii)考虑轮状病毒疫苗接种覆盖率;(iv)将轮状病毒阳性比例转换为轮状病毒归因分数;以及(v)计算不确定性范围值。我们开展了新的分析以指导未来的估计。基于9个国家84个医院的数据,我们发现急性水样腹泻与5岁以下儿童腹泻住院病例的87%(95%置信区间83 - 90%)有关;基于9个国家地区的口头尸检报告,急性水样腹泻与5岁以下儿童腹泻死亡病例的65%(95%置信区间57 - 74%)有关。我们重新分析了全球肠道多中心研究(GEMS)的数据,发现在5岁以下儿童急性水样腹泻住院病例中,轮状病毒阳性率为44%(亚洲为55%,非洲为32%),在5岁以下儿童急性水样腹泻死亡病例中,轮状病毒阳性率为28%。检测出轮状病毒呈阳性的5岁以下儿童腹泻住院病例中,97%(95%置信区间95 - 98%)完全归因于轮状病毒。对于所有合并的临床综合征,轮状病毒归因分数为34%(95%置信区间31 - 36%)。当使用更灵敏的分子检测方法重新分析GEMS结果时,该分数增加了1.08倍(95%置信区间1.02 - 1.14)。
我们就提高未来轮状病毒死亡率估计的质量和透明度的七项提议达成了共识。