Tridente Ascanio, Bion Julian, Mills Gary H, Gordon Anthony C, Clarke Geraldine M, Walden Andrew, Hutton Paula, Holloway Paul A H, Chiche Jean-Daniel, Stuber Frank, Garrard Christopher, Hinds Charles
Whiston Hospital Prescot, Merseyside and Department of Infection, Immunity and Cardiovascular Disease, The Medical School, University of Sheffield, Sheffield, UK.
School of Clinical and Experimental Medicine, University of Birmingham, Birmingham, UK.
Ann Intensive Care. 2017 Sep 12;7(1):96. doi: 10.1186/s13613-017-0314-1.
Prognostic scores and models of illness severity are useful both clinically and for research. The aim of this study was to develop two prognostic models for the prediction of long-term (6 months) and 28-day mortality of postoperative critically ill patients with faecal peritonitis (FP).
Patients admitted to intensive care units with faecal peritonitis and recruited to the European GenOSept study were divided into a derivation and a geographical validation subset; patients subsequently recruited to the UK GAinS study were used for temporal validation. Using all 50 clinical and laboratory variables available on day 1 of critical care admission, Cox proportional hazards regression was fitted to select variables for inclusion in two prognostic models, using stepwise selection and nonparametric bootstrapping sampling techniques. Using Area under the receiver operating characteristic curve (AuROC) analysis, the performance of the models was compared to SOFA and APACHE II.
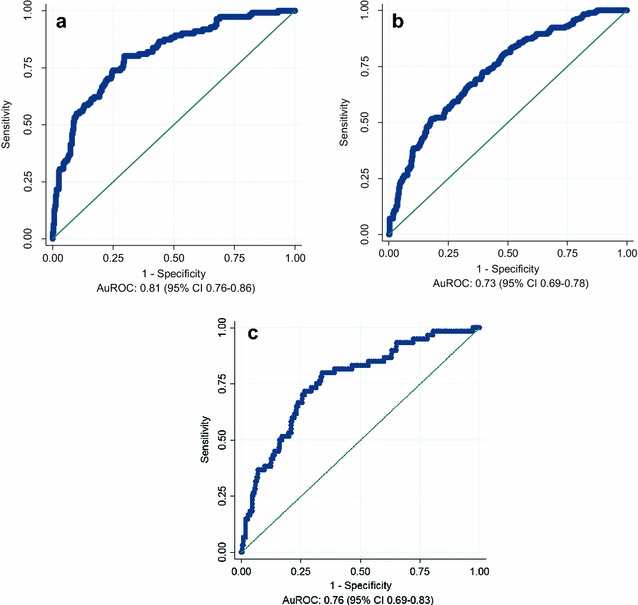
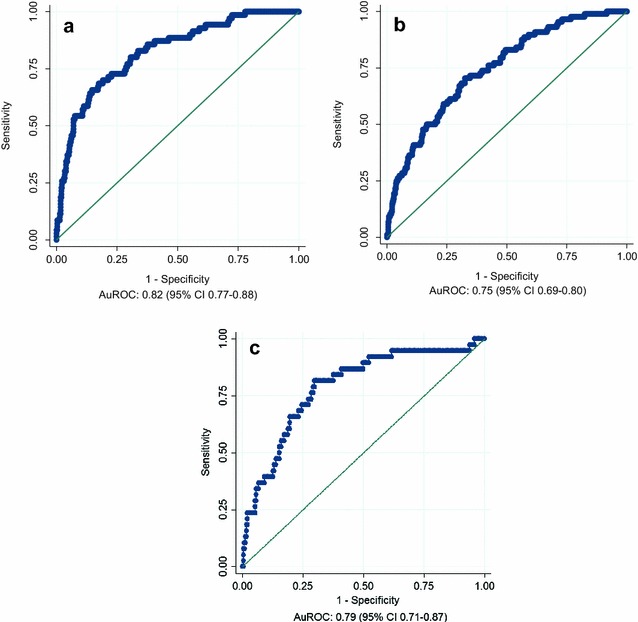
Five variables (age, SOFA score, lowest temperature, highest heart rate, haematocrit) were entered into the prognostic models. The discriminatory performance of the 6-month prognostic model yielded an AuROC 0.81 (95% CI 0.76-0.86), 0.73 (95% CI 0.69-0.78) and 0.76 (95% CI 0.69-0.83) for the derivation, geographic and temporal external validation cohorts, respectively. The 28-day prognostic tool yielded an AuROC 0.82 (95% CI 0.77-0.88), 0.75 (95% CI 0.69-0.80) and 0.79 (95% CI 0.71-0.87) for the same cohorts. These AuROCs appeared consistently superior to those obtained with the SOFA and APACHE II scores alone.
The two prognostic models developed for 6-month and 28-day mortality prediction in critically ill septic patients with FP, in the postoperative phase, enhanced the day one SOFA score's predictive utility by adding a few key variables: age, lowest recorded temperature, highest recorded heart rate and haematocrit. External validation of their predictive capability in larger cohorts is needed, before introduction of the proposed scores into clinical practice to inform decision making and the design of clinical trials.
预后评分和疾病严重程度模型在临床和研究中均有用处。本研究的目的是开发两种预后模型,用于预测术后患有粪性腹膜炎(FP)的危重症患者的长期(6个月)和28天死亡率。
纳入欧洲GenOSept研究的入住重症监护病房的粪性腹膜炎患者被分为一个推导子集和一个地理验证子集;随后纳入英国GAinS研究的患者用于时间验证。利用重症监护入院第1天可用的所有50项临床和实验室变量,采用逐步选择和非参数自助抽样技术,拟合Cox比例风险回归以选择纳入两个预后模型的变量。使用受试者工作特征曲线下面积(AuROC)分析,将模型的性能与序贯器官衰竭评估(SOFA)和急性生理与慢性健康状况评分系统II(APACHE II)进行比较。
五个变量(年龄、SOFA评分、最低体温、最高心率、血细胞比容)被纳入预后模型。6个月预后模型的辨别性能在推导、地理和时间外部验证队列中分别产生AuROC为0.81(95%可信区间0.76 - 0.86)、0.73(95%可信区间0.69 - 0.78)和0.76(95%可信区间0.69 - 0.83)。28天预后工具在相同队列中产生AuROC为0.82(95%可信区间0.77 - 0.88)、0.75(95%可信区间0.69 - 0.80)和0.79(95%可信区间0.71 - 0.87)。这些AuROC始终优于单独使用SOFA和APACHE II评分所获得的值。
为预测术后患有FP的脓毒症危重症患者的6个月和28天死亡率而开发的两种预后模型,通过添加几个关键变量:年龄、记录的最低体温、记录的最高心率和血细胞比容,增强了第1天SOFA评分的预测效用。在将建议的评分引入临床实践以指导决策和设计临床试验之前,需要在更大队列中对其预测能力进行外部验证。