Tsujino Daisuke, Nishimura Rimei, Onda Yoshiko, Seo Chiaki, Ando Kiyotaka, Utsunomiya Kazunori
Division of Diabetes, Metabolism and Endocrinology, Department of Internal Medicine, Jikei University School of Medicine, Tokyo, Japan.
J Diabetes Investig. 2017 Sep 16;9(3):573-8. doi: 10.1111/jdi.12747.
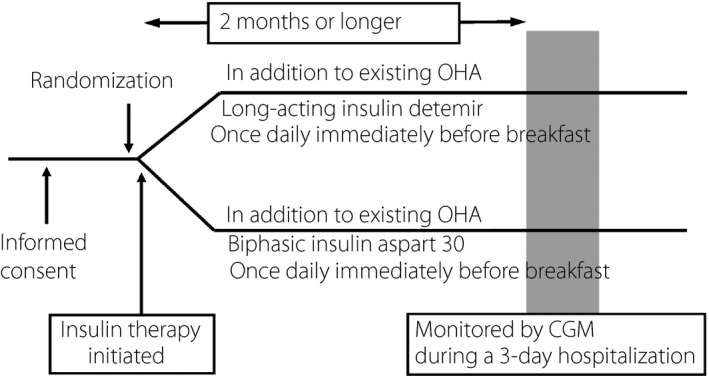
We compared the efficacy of insulin detemir and biphasic insulin aspart-30 given in the morning as an add-on to oral hypoglycemic agents in type 2 diabetes patients.
The present study enrolled 30 patients with poorly controlled type 2 diabetes (8% ≤ glycated hemoglobin < 11%) being treated with oral hypoglycemic agent mono- or combination therapy with biguanides, sulfonylureas or thiazolidinediones. The patients were randomly assigned to insulin detemir (group D) or insulin aspart-30 (group A) given in the morning as add-on to oral hypoglycemic agents. After adjusting their insulin doses, the patients that underwent continuous glucose monitoring during a 3-day hospitalization and with day 2 continuous glucose monitoring data were subjected to analysis.
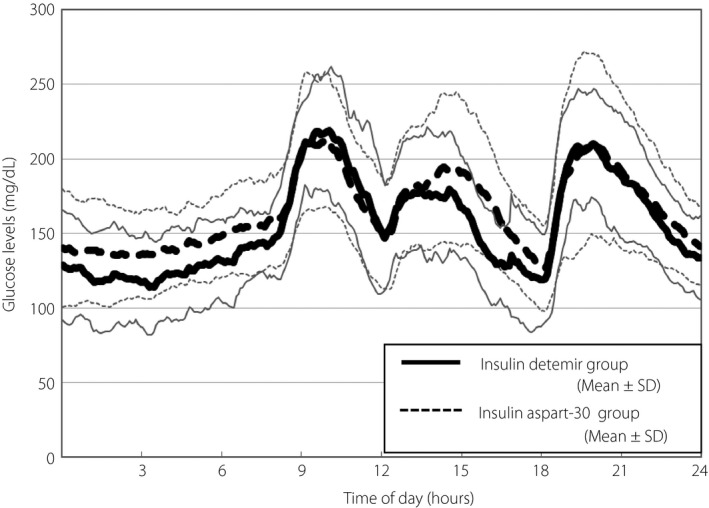
There was no significant difference in patient background, baseline glycated hemoglobin levels and insulin doses during continuous glucose monitoring between the two groups. The percent coefficient of variation of 24-h glucose levels was significantly lower in group A (20.4 ± 7.6) than in group D (27.1 ± 6.5; P = 0.015). Similarly, mean amplitude of glycemic excursions was significantly smaller in group A (80 ± 32) than in group D (102 ± 14; P = 0.021). Postprandial glucose excursions were significantly smaller after breakfast in group A (65 ± 31 mg/dL) than in group D (106 ± 32 mg/dL; P = 0.002).
As once-daily insulin injection therapy given before breakfast in type 2 diabetes patients, the biphasic insulin analog might represent a better insulin option in significantly lowering the percent coefficient of variation and mean amplitude of glycemic excursions than the long-acting insulin preparation.
我们比较了在2型糖尿病患者中,将德谷胰岛素与门冬胰岛素30在早晨作为口服降糖药的补充用药的疗效。
本研究纳入了30例2型糖尿病控制不佳(糖化血红蛋白8%≤糖化血红蛋白<11%)的患者,这些患者正在接受口服降糖药单药治疗或与双胍类、磺脲类或噻唑烷二酮类联合治疗。患者被随机分配接受德谷胰岛素(D组)或门冬胰岛素30(A组),早晨作为口服降糖药的补充用药。调整胰岛素剂量后,在3天住院期间进行持续葡萄糖监测且有第2天持续葡萄糖监测数据的患者接受分析。
两组患者的背景、基线糖化血红蛋白水平和持续葡萄糖监测期间的胰岛素剂量无显著差异。A组24小时血糖水平的变异系数百分比(20.4±7.6)显著低于D组(27.1±6.5;P=0.015)。同样,A组血糖波动平均幅度(80±32)显著小于D组(102±14;P=0.021)。早餐后A组餐后血糖波动(65±31mg/dL)显著小于D组(106±32mg/dL;P=0.002)。
作为2型糖尿病患者早餐前每日一次的胰岛素注射治疗,双相胰岛素类似物可能比长效胰岛素制剂在显著降低血糖变异系数百分比和血糖波动平均幅度方面是更好的胰岛素选择。