Rigault Eugénie, Lenoir Laurence, Bouguen Guillaume, Pagenault Mael, Lièvre Astrid, Garin Etienne, Siproudhis Laurent, Bretagne Jean-François
Service des Maladies de l'Appareil Digestif, Hôpital Pontchaillou, Centre Hospitalo-Universitaire, Rennes.
Service de Médecine Nucléaire, Centre Eugène Marquis, Rennes.
Endosc Int Open. 2017 Sep;5(9):E924-E930. doi: 10.1055/s-0043-116384. Epub 2017 Sep 13.
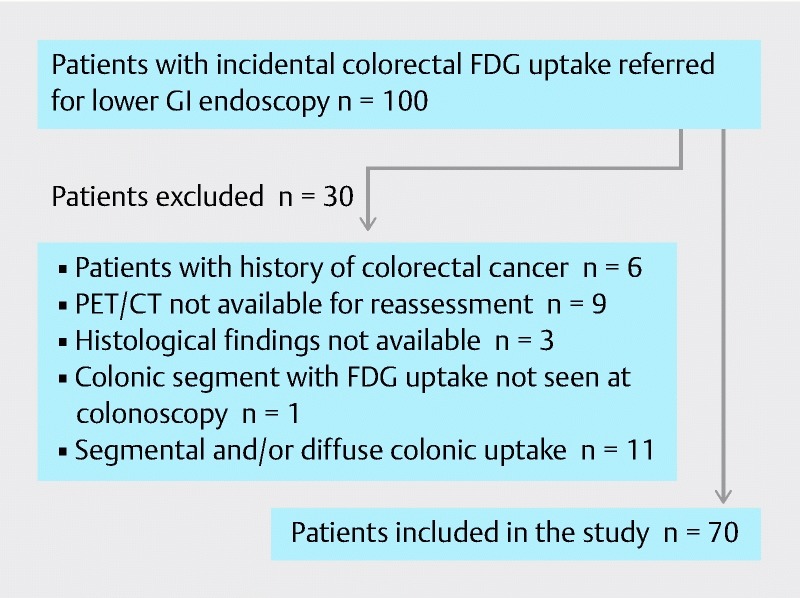
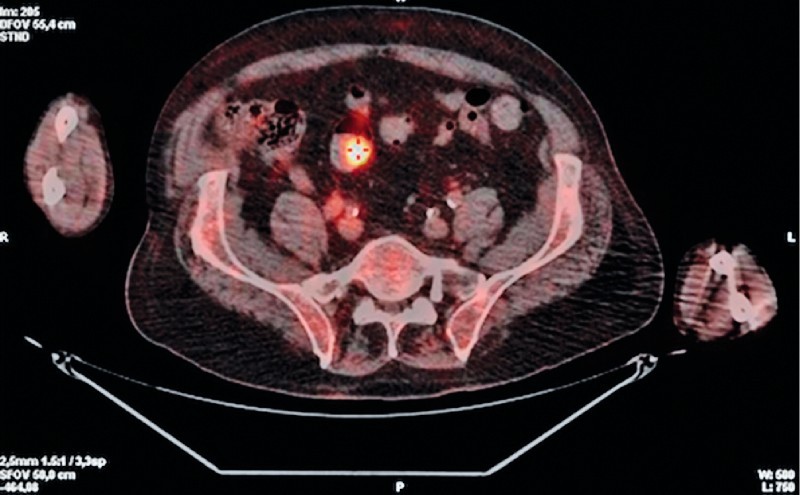
The relevance of incidental colorectal focal F-FDG PET/CT uptake is debatable. All patients who were referred for colonoscopy because of incidental colonic focal FDG uptake were included in this retrospective study.
PET/CT imaging characteristics were reviewed by a nuclear physician who was blinded to endoscopic and histopathological findings to determine the location of FDG uptake sites and to measure the maximum standardized uptake values (SUVmax) and metabolic volume (MV). Endoscopic findings were categorized as malignant lesions (ML), high-risk polyps (HRP), low-risk polyps (LRP) or other non-neoplastic lesions (NNL).
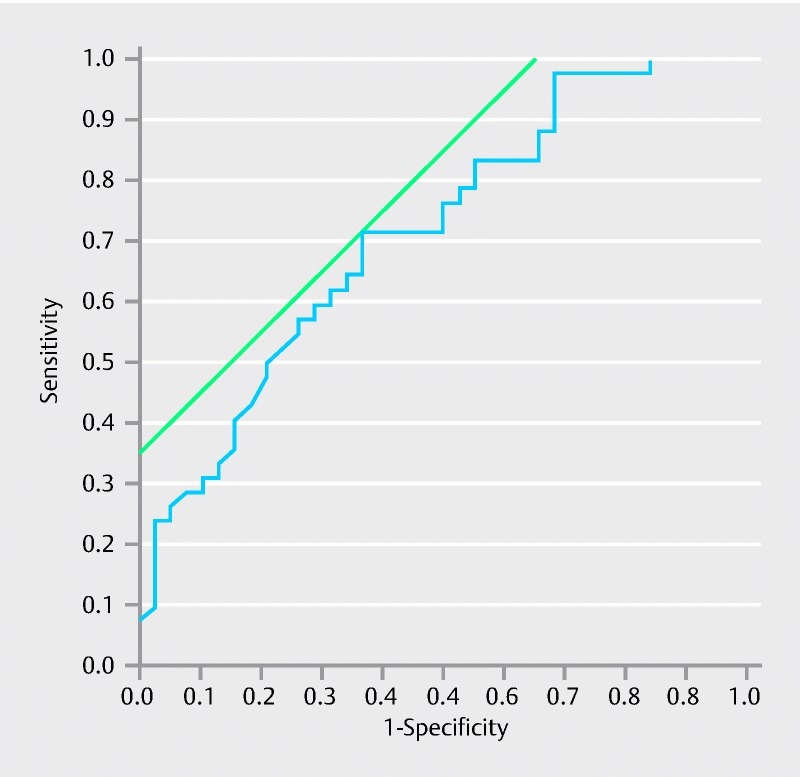
Seventy patients with 84 foci of FDG uptake were included. The proportions of true-positive (lesions found at colonoscopy at the same location) and false-positive (no lesion at colonoscopy) PET/CT findings were 65.5 % (n = 55) and 34.5 % (n = 29). Median SUVmax values did not differ between true-positive and false-positive findings ( = 0.27). Median MV30 values differed significantly between true-positive (5.5 cm , [3.3 - 10.9 cm ]) and false-positive (9.7 cm , [5.2 - 40.8 cm ]) findings ( = 0.015). Among the 55 true-positive FDG uptake sites, there were 14 (25.5 %) malignant lesions, 30 (54.5 %) HRP, 4 (7.3 %) LRP, and 7 (12.7 %) NNL. Median MV30 values differed significantly between advanced neoplasia (5.0 cm , [2.9 - 9.7 cm ]) and other endoscopic findings (9.4 cm , [5.2 - 39.8 cm ]) ( = 0.001); the AUROC was 0.71. By per-colonic segment analysis, the distribution of true-positive, false-negative, false-positive, and true-negative FDG PET/CT findings was as follows: 21.5 %, 14.2 %, 11.5 %, and 52.8 %, respectively.
Our study demonstrates that follow-up complete colonoscopy is mandatory in all patients with incidental colorectal focal F-FDG PET/CT uptake.
结直肠FDG摄取灶的相关性存在争议。本回顾性研究纳入了所有因结直肠FDG摄取灶而接受结肠镜检查的患者。
由一位对内镜及组织病理学结果不知情的核医学医师回顾PET/CT影像特征,以确定FDG摄取部位的位置,并测量最大标准化摄取值(SUVmax)和代谢体积(MV)。内镜检查结果分为恶性病变(ML)、高危息肉(HRP)、低危息肉(LRP)或其他非肿瘤性病变(NNL)。
纳入了70例有84个FDG摄取灶的患者。PET/CT检查结果的真阳性(结肠镜检查在相同位置发现病变)和假阳性(结肠镜检查未发现病变)比例分别为65.5%(n = 55)和34.5%(n = 29)。真阳性和假阳性结果的SUVmax中位数无差异(P = 0.27)。真阳性(5.5 cm³,[3.3 - 10.9 cm³])和假阳性(9.7 cm³,[5.2 - 40.8 cm³])结果的MV30中位数有显著差异(P = 0.015)。在55个真阳性FDG摄取部位中,有14个(25.5%)为恶性病变,30个(54.5%)为HRP,4个(7.3%)为LRP,7个(12.7%)为NNL。进展期肿瘤(5.0 cm³,[2.9 - 9.7 cm³])和其他内镜检查结果(9.4 cm³,[5.2 - 39.8 cm³])的MV30中位数有显著差异(P = 0.001);曲线下面积为0.71。按结肠节段分析,FDG PET/CT检查结果的真阳性、假阴性、假阳性和真阴性分布分别为21.5%、14.2%、11.5%和52.8%。
我们的研究表明,所有结直肠FDG摄取灶患者均必须进行全结肠镜随访。