Matthews Veronica, Burgess Christopher P, Connors Christine, Moore Elizabeth, Peiris David, Scrimgeour David, Thompson Sandra C, Larkins Sarah, Bailie Ross
The University of Sydney, University Centre for Rural Health - North Coast, Lismore, NSW, Australia.
Top End Health Service, Northern Territory Government, Darwin, NT, Australia.
Front Public Health. 2017 Sep 4;5:233. doi: 10.3389/fpubh.2017.00233. eCollection 2017.
Aboriginal and Torres Strait Islander Australians experience a greater burden of disease compared to non-Indigenous Australians. Around one-fifth of the health disparity is caused by cardiovascular disease (CVD). Despite the importance of absolute cardiovascular risk assessment (CVRA) as a screening and early intervention tool, few studies have reported its use within the Australian Indigenous primary health care (PHC) sector. This study utilizes data from a large-scale quality improvement program to examine variation in documented CVRA as a primary prevention strategy for individuals without prior CVD across four Australian jurisdictions. We also examine the proportion with elevated risk and follow-up actions recorded.
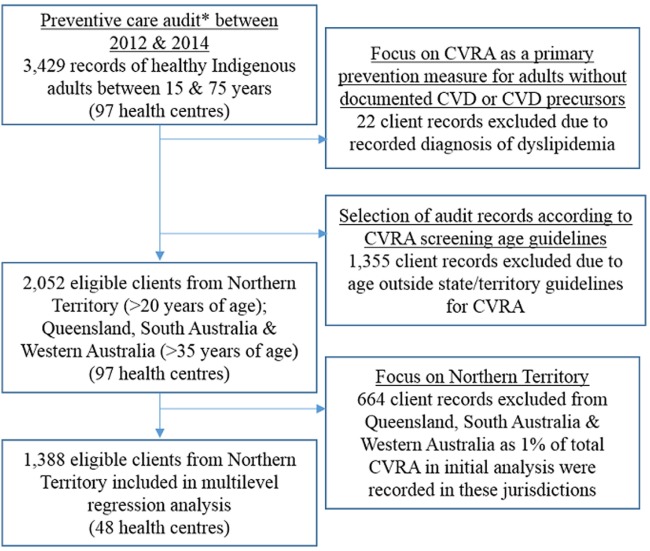
We undertook cross-sectional analysis of 2,052 client records from 97 PHC centers to assess CVRA in Indigenous adults aged ≥20 years with no recorded chronic disease diagnosis (2012-2014). Multilevel regression was used to quantify the variation in CVRA attributable to health center and client level factors. The main outcome measure was the proportion of eligible adults who had CVRA recorded. Secondary outcomes were the proportion of clients with elevated risk that had follow-up actions recorded.
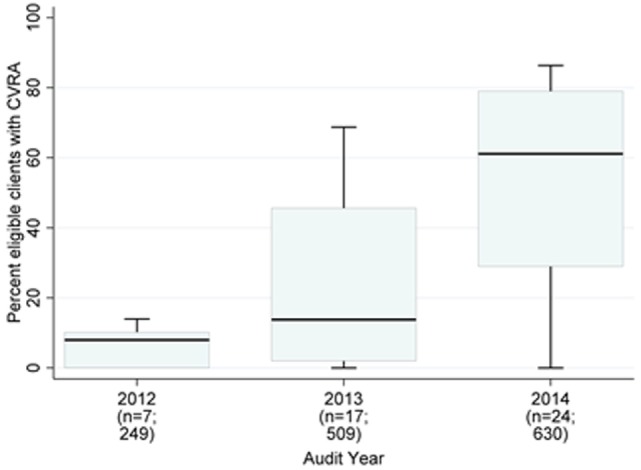
Approximately 23% ( = 478) of eligible clients had documented CVRA. Almost all assessments (99%) were conducted in the Northern Territory. Within this jurisdiction, there was wide variation between centers in the proportion of clients with documented CVRA (median 38%; range 0-86%). Regression analysis showed health center factors accounted for 48% of the variation. Centers with integrated clinical decision support systems were more likely to document CVRA (OR 21.1; 95% CI 5.4-82.4; < 0.001). Eleven percent ( = 53) of clients were found with moderate/high CVD risk, of whom almost one-third were under 35 years ( = 16). Documentation of follow-up varied with respect to the targeted risk factor. Fewer than 30% with abnormal blood lipid or glucose levels had follow-up management plans recorded.
There was wide variation in CVRA between jurisdictions and between PHC centers. Learnings from successful interventions to educate and support centers in CVRA provision should be shared with stakeholders more widely. Where risk has been identified, further improvement in follow-up management is required to prevent CVD onset and reduce future burden in Australia's Indigenous population.
与非澳大利亚原住民相比,澳大利亚原住民和托雷斯海峡岛民承受着更大的疾病负担。约五分之一的健康差距是由心血管疾病(CVD)导致的。尽管绝对心血管风险评估(CVRA)作为一种筛查和早期干预工具很重要,但很少有研究报告其在澳大利亚原住民初级卫生保健(PHC)部门的使用情况。本研究利用一项大规模质量改进项目的数据,来检查在四个澳大利亚司法管辖区内,作为对无既往CVD个体的一级预防策略,记录在案的CVRA的差异。我们还检查了风险升高及记录的后续行动的比例。
我们对来自97个初级卫生保健中心的2052份客户记录进行横断面分析,以评估年龄≥20岁且无慢性疾病诊断记录的原住民成年人的CVRA(2012 - 2014年)。使用多水平回归来量化归因于卫生中心和客户层面因素的CVRA差异。主要结局指标是有CVRA记录的符合条件成年人的比例。次要结局是有后续行动记录的风险升高客户的比例。
约23%(n = 478)符合条件的客户有记录在案的CVRA。几乎所有评估(99%)都在北领地进行。在该司法管辖区内,有记录在案的CVRA的客户比例在各中心之间存在很大差异(中位数38%;范围0 - 86%)。回归分析表明,卫生中心因素占差异的48%。拥有综合临床决策支持系统的中心更有可能记录CVRA(OR 21.1;95% CI 5.4 - 82.4;P < 0.001)。发现有百分之十一(n = 53)的客户存在中度/高度CVD风险,其中近三分之一年龄在35岁以下(n = 16)。后续行动的记录因目标风险因素而异。血脂或血糖水平异常的客户中,记录有后续管理计划的不到30%。
各司法管辖区之间以及初级卫生保健中心之间的CVRA存在很大差异。应更广泛地与利益相关者分享成功干预措施的经验教训,以教育和支持各中心提供CVRA。在已识别出风险的情况下,需要进一步改进后续管理,以预防CVD发病并减轻澳大利亚原住民未来的负担。