Kavsak Peter A, Beattie John, Pickersgill Robin, Ford Lynn, Caruso Nadia, Clark Lorna
Department of Pathology and Molecular Medicine, McMaster University, Hamilton, ON, Canada.
Juravinski Hospital and Cancer Centre, Hamilton, Canada.
Pract Lab Med. 2015 Mar 3;1:28-34. doi: 10.1016/j.plabm.2015.02.001. eCollection 2015 Apr 1.
Despite several publications on the analytical performance of high-sensitivity cardiac troponin (hs-cTn) assays, there has been little information on how laboratories should validate and implement these assays into clinical service. Our study provides a practical approach for the validation and implementation of a hs-cTn assay across a large North American City.
Validation for the Abbott ARCHITECT hs-cTnI assay (across 5 analyzers) consisted of verification of limit of blank (LoB), precision (i.e., coefficient of variation; CV) testing at the reported limit of detection (LoD) and within and outside the 99th percentile, linearity testing, cTnI versus hs-cTnI patient comparison within and between analyzers (Passing and Bablok and non-parametric analyses). Education, clinical communications, and memorandums were issued in advance to inform all staff across the city as well as a selected reminder the day before live-date to important users. All hospitals switched to the hs-cTnI assay concurrently (the contemporary cTnI assay removed) with laboratory staff instructed to repeat samples previously measured with the contemporary cTnI assay with the hs-cTnI assay only by physician request.
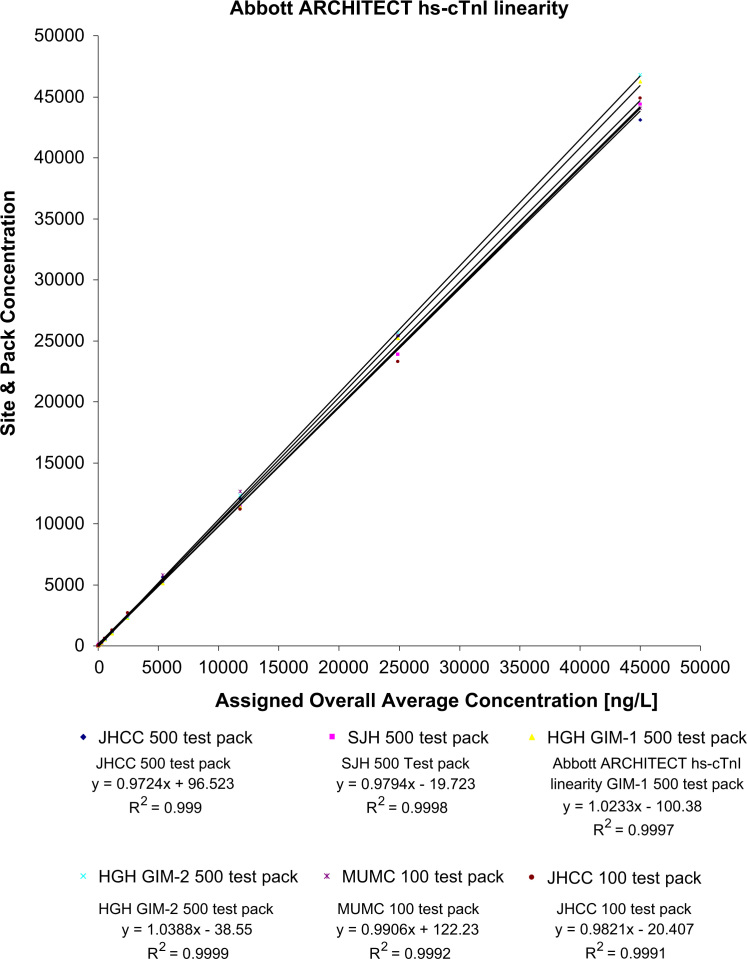
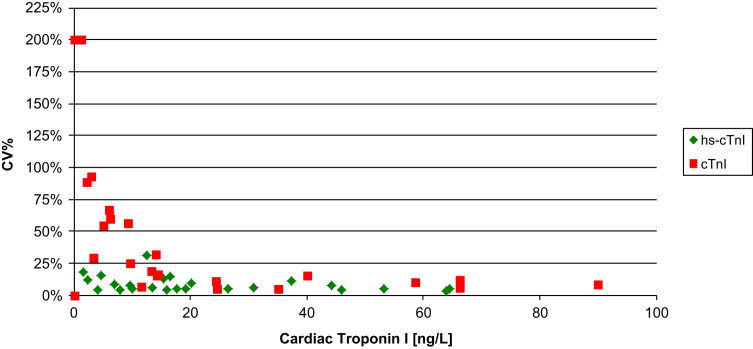
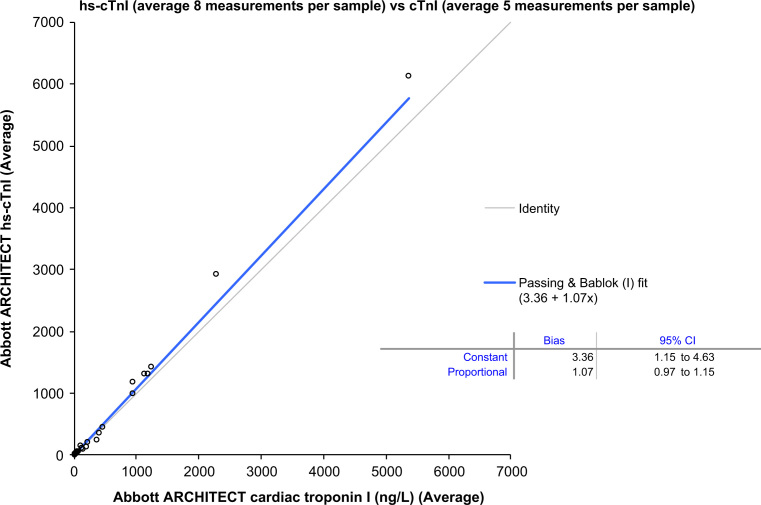
Across the 5 analyzers and 6 reagent packs the overall LoB was 0.6 ng/L (=60) with a CV of 33% at an overall mean of 1.2 ng/L (=60; reported LoD=1.0 ng/L), with linearity demonstrated from 45,005 ng/L to 1.1 ng/L. Precision testing with a normal patient-pool QC material (mean range across 5 analyzers was 3.9-4.4 ng/L) yielded a range of CVs from 7% to 10% (within-run) and CVs from 7% to 18% (between-run) with the high patient-pool QC material (mean range across 5 analyzers was 29.6-36.3 ng/L) yielding a range of CVs from 2% to 5% (within-run) and CVs from 4% to 8% (between-run). There was agreement between hs-cTnI versus cTnI with the patient samples (slope ranges: 0.89-1.03; intercept ranges: 1.9-3.8 ng/L), however, the median CV on patient samples <100 ng/L across the analyzers was 5.6% for hs-cTnI versus 18.7% for the contemporary assay (<0.001). Following the switch to hs-cTnI testing, no requests for repeat measurements were received.
Validation and implementation of hs-cTnI testing across multiple sites requires collaboration within the laboratories and between hospital laboratories and clinical staff.
尽管已有多篇关于高敏心肌肌钙蛋白(hs-cTn)检测分析性能的文献,但关于实验室应如何验证这些检测方法并将其应用于临床服务的信息却很少。我们的研究为在北美一个大城市中验证和实施hs-cTn检测提供了一种实用方法。
对雅培ARCHITECT hs-cTnI检测(在5台分析仪上)的验证包括空白限(LoB)验证、在报告的检测限(LoD)以及第99百分位数之内和之外进行精密度(即变异系数;CV)测试、线性测试、分析仪内部和之间cTnI与hs-cTnI患者样本比较(Passing和Bablok以及非参数分析)。提前发布教育资料、临床沟通内容和备忘录,告知全市所有工作人员,并在启用前一天向重要用户发送选定的提醒信息。所有医院同时切换到hs-cTnI检测(停用当代cTnI检测),实验室工作人员仅在医生要求时,才用hs-cTnI检测重复先前用当代cTnI检测测量过的样本。
在5台分析仪和6个试剂包中,总体LoB为0.6 ng/L(=60),在总体均值1.2 ng/L(=60;报告LoD = 1.0 ng/L)时CV为33%,线性范围为45,005 ng/L至1.1 ng/L。用正常患者池质量控制材料进行精密度测试(5台分析仪的平均范围为3.9 - 4.4 ng/L),批内CV范围为7%至10%,批间CV范围为7%至18%;用高患者池质量控制材料(5台分析仪的平均范围为29.6 - 36.3 ng/L),批内CV范围为2%至5%,批间CV范围为4%至8%。hs-cTnI与cTnI在患者样本上具有一致性(斜率范围:0.89 - 1.03;截距范围:1.9 - 3.8 ng/L),然而,分析仪上hs-cTnI在<100 ng/L患者样本上的中位CV为5.6%,而当代检测为18.7%(<0.001)。切换到hs-cTnI检测后,未收到重复测量的请求。
在多个地点验证和实施hs-cTnI检测需要实验室内部以及医院实验室与临床工作人员之间的协作。