Acute and Chronic Renal Failure Unit, Department of Clinical and Experimental Medicine Renal ICU, Parma University Hospital, Parma 43126, Italy.
Department of General Intensive Care and Institute for Nutrition Research, Rabin Medical Center, Beilinson Hospital, Petah Tikva, Affiliated with the Sackler School of Medicine, Tel Aviv University, Tel Aviv 49100, Israel.
Nutrients. 2017 Jul 26;9(8):802. doi: 10.3390/nu9080802.
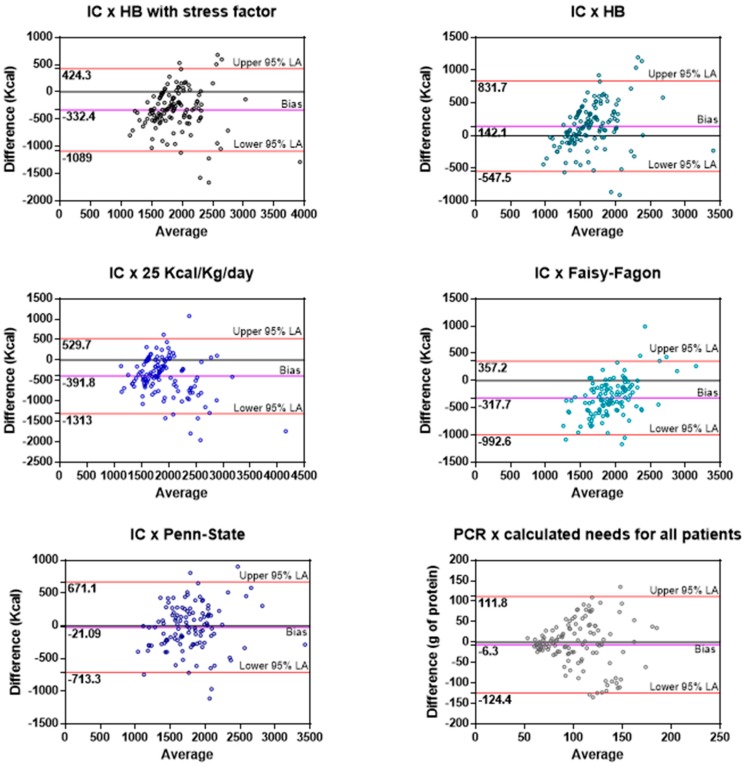
The optimal nutritional support in Acute Kidney Injury (AKI) still remains an open issue. The present study was aimed at evaluating the validity of conventional predictive formulas for the calculation of both energy expenditure and protein needs in critically ill patients with AKI. A prospective, multicenter, observational study was conducted on adult patients hospitalized with AKI in three different intensive care units (ICU). Nutrient needs were estimated by different methods: the Guidelines of the European Society of Parenteral and Enteral Nutrition (ESPEN) for both calories and proteins, the Harris-Benedict equation, the Penn-State and Faisy-Fagon equations for energy. Actual energy and protein needs were repeatedly measured by indirect calorimetry (IC) and protein catabolic rate (PCR) until oral nutrition start, hospital discharge or renal function recovery. Forty-two patients with AKI were enrolled, with 130 IC and 123 PCR measurements obtained over 654 days of artificial nutrition. No predictive formula was precise enough, and Bland-Altman plots wide limits of agreement for all equations highlight the potential to under- or overfeed individual patients. Conventional predictive formulas may frequently lead to incorrect energy and protein need estimation. In critically ill patients with AKI an increased risk for under- or overfeeding is likely when nutrient needs are estimated instead of measured.
急性肾损伤(AKI)的最佳营养支持仍然是一个悬而未决的问题。本研究旨在评估传统预测公式计算 AKI 危重症患者能量和蛋白质需求的有效性。一项前瞻性、多中心、观察性研究在三个不同的重症监护病房(ICU)对 AKI 住院的成年患者进行了研究。营养需求通过不同方法进行估计:ESPEN 指南(欧洲肠外和肠内营养学会)分别用于热量和蛋白质,Harris-Benedict 方程,Penn-State 和 Faisy-Fagon 方程用于能量。实际能量和蛋白质需求通过间接热量法(IC)和蛋白质分解率(PCR)反复测量,直到开始口服营养、出院或肾功能恢复。共纳入 42 例 AKI 患者,在 654 天的人工营养期间共获得 130 次 IC 和 123 次 PCR 测量。没有一种预测公式足够精确,所有方程的 Bland-Altman 图显示了协议范围较宽,这突出了个体患者可能出现喂养不足或过度的潜在风险。传统的预测公式可能经常导致能量和蛋白质需求估计不准确。在 AKI 危重症患者中,当通过估计而不是测量来确定营养需求时,患者可能面临喂养不足或过度的风险增加。