Jung Sung Woo, Park In Ja, Oh Se Heon, Yeom Seung-Seop, Lee Jong Lyul, Yoon Yong Sik, Kim Chan Wook, Lim Seok-Byung, Lee Jung Bok, Yu Chang Sik, Kim Jin Cheon
Department of Colon and Rectal Surgery, University of Ulsan College of Medicine and Asan Medical Center, Seoul, Korea.
Department of Clinical Epidemiology and Biostatistics, University of Ulsan College of Medicine and Asan Medical Center, Seoul, Korea.
Oncotarget. 2017 Feb 27;8(35):59757-59765. doi: 10.18632/oncotarget.15760. eCollection 2017 Aug 29.
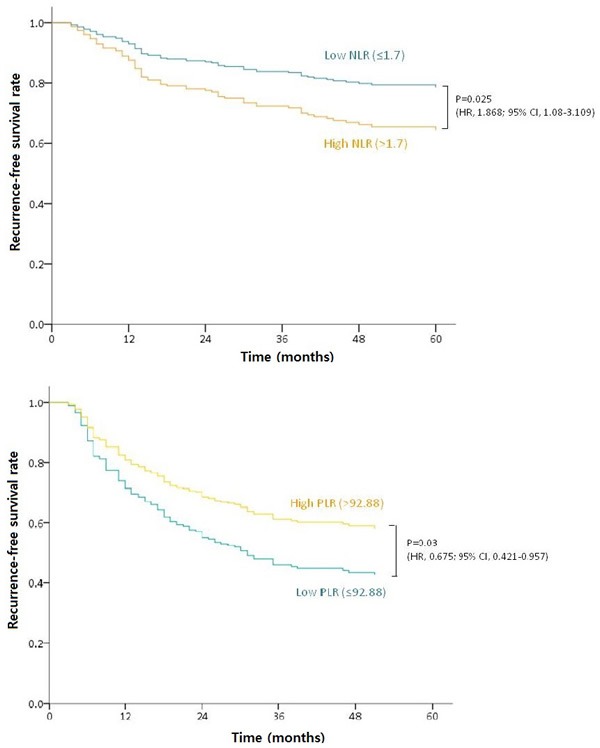
We investigated retrospectively whether immunologic markers from a complete blood count (CBC) are associated with the responsiveness to preoperative chemoradiotherapy (PCRT) and oncologic outcomes in 984 patients with locally advanced rectal cancer (LARC) who also underwent radical surgery from 2005 to 2013. CBC parameters including the neutrophil to lymphocyte ratio (NLR), lymphocyte to monocyte ratio (LMR), and platelet to lymphocyte ratio (PLR) were recorded. Pathologic responses to PCRT were evaluated in the resected specimens using the tumor regression grade system. The cut-off values of the immunologic markers were calculated to analyze their association with recurrence-free survival (RFS). One hundred ninety-five patients achieved total regression of their primary tumor. By receiver operating characteristic analysis, NLR, PLR, and LMR could not distinguish total regression from residual disease after PCRT. The NLR, LMR and PLR cut-off values were 1.7, 6.8 and 92.88, respectively. By univariate analysis, low NLR (≤1.7), high LMR (>6.8) and high PLR (>92.88) were indicators of a favorable RFS outcome. By multivariate analysis, high PLR was associated with an improved RFS (HR, 0.649; 95% CI, 0.473-0.89; =0.007). High NLR (>1.7) was an independent negative prognostic factor for RFS in stage II (HR, 1.868; 95% CI, 1.08-3.109; =0.025) and high PLR was a positive prognostic factor in stage III (HR, 0.675; 95% CI, 0.421-0.957; =0.03). Immunologic markers derived from CBCs are independently associated with the RFS outcome in LARC patients treated with PCRT followed by radical resection. However, these markers are not predictive of total primary tumor regression after PCRT.
我们回顾性研究了984例2005年至2013年间接受根治性手术的局部晚期直肠癌(LARC)患者全血细胞计数(CBC)中的免疫标志物是否与术前放化疗(PCRT)的反应性及肿瘤学结局相关。记录了包括中性粒细胞与淋巴细胞比值(NLR)、淋巴细胞与单核细胞比值(LMR)以及血小板与淋巴细胞比值(PLR)在内的CBC参数。使用肿瘤退缩分级系统在切除标本中评估对PCRT的病理反应。计算免疫标志物的临界值以分析其与无复发生存期(RFS)的关联。195例患者实现了原发肿瘤的完全退缩。通过受试者工作特征分析,NLR、PLR和LMR无法区分PCRT后完全退缩与残留疾病。NLR、LMR和PLR的临界值分别为1.7、6.8和92.88。单因素分析显示,低NLR(≤1.7)、高LMR(>6.8)和高PLR(>92.88)是RFS结局良好的指标。多因素分析显示,高PLR与RFS改善相关(HR,0.649;95%CI,0.473 - 0.89;P = 0.007)。高NLR(>1.7)是II期RFS的独立阴性预后因素(HR,1.868;95%CI,1.08 - 3.109;P = 0.025),高PLR是III期的阳性预后因素(HR,0.675;95%CI,0.421 - 0.957;P = 0.03)。源自CBC的免疫标志物与接受PCRT后行根治性切除的LARC患者的RFS结局独立相关。然而,这些标志物不能预测PCRT后原发肿瘤的完全退缩。