Holm Solrun G, Mathisen Terje A, Sæterstrand Torill M, Brinchmann Berit S
Faculty of Nursing and Health Sciences, Nord University, Storgt 105, 8370, Leknes, Norway.
Nord University Business School, 8049, Bodø, Norway.
BMC Health Serv Res. 2017 Sep 22;17(1):673. doi: 10.1186/s12913-017-2623-3.
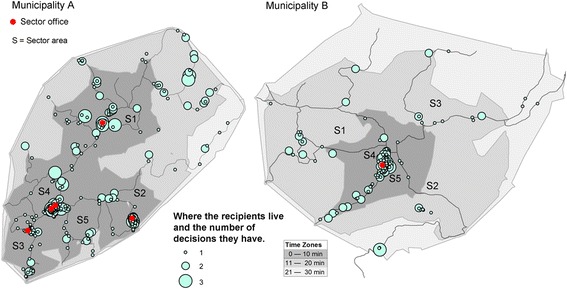
In Norway, elder care is primarily a municipal responsibility. Municipal health services strive to offer the 'lowest level of effective care,' and home healthcare services are defined as the lowest level of care in Norway. Municipalities determine the type(s) of service and the amount of care applicants require. The services granted are outlined in an individual decision letter, which serves as a contract between the municipality and the home healthcare recipient. The purpose of this study was to gain insight into the scope and duration of home healthcare services allocated by municipalities and to determine where home care recipients live in relation to home healthcare service offices.
A document analysis was performed on data derived from 833 letters to individuals allocated home care services in two municipalities in Northern Norway (Municipality A = 500 recipients, Municipality B = 333 recipients).
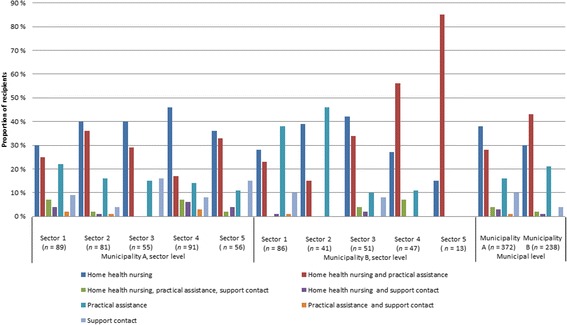
In Municipality A, 74% of service hours were allotted to home health nursing, 12% to practical assistance, and 14% to support contact; in Municipality B, the distribution was 73%, 19%, and 8%, respectively. Both municipalities allocated home health services with no service end date (41% and 85% of the total services, respectively). Among recipients of "expired" services, 25% in Municipality A and 7% in Municipality B continued to receive assistance.
Our findings reveal that the municipalities adhered to the goal for home care recipients to remain at home as long as possible before moving into a nursing home. The findings also indicate that the system for allocating home healthcare services may not be fair, as the municipalities lacked procedures for revising individual decisions. Our findings indicate that local authorities should closely examine how they design individual decisions and increase their awareness of how long a service should be provided.
在挪威,老年护理主要由市政当局负责。市政卫生服务机构努力提供“最低水平的有效护理”,家庭医疗服务被定义为挪威护理的最低水平。市政当局决定服务类型和申请人所需护理量。所提供的服务在一份个人决定书里列出,该决定书作为市政当局与家庭医疗服务接受者之间的合同。本研究的目的是深入了解市政当局分配的家庭医疗服务的范围和时长,并确定家庭护理接受者相对于家庭医疗服务办公室的居住地点。
对挪威北部两个市政当局(市政当局A = 500名接受者,市政当局B = 333名接受者)向个人分配家庭护理服务的833封信函中的数据进行了文献分析。
在市政当局A,74%的服务时长分配给了家庭健康护理,12%用于实际协助,14%用于支持性联系;在市政当局B,分配比例分别为73%、19%和8%。两个市政当局分配的家庭健康服务均无服务结束日期(分别占总服务的41%和85%)。在“已过期”服务的接受者中,市政当局A有25%、市政当局B有7%继续接受援助。
我们的研究结果表明,市政当局坚持让家庭护理接受者在搬进养老院之前尽可能长时间居家的目标。研究结果还表明,家庭医疗服务分配系统可能不公平,因为市政当局缺乏修订个人决定的程序。我们的研究结果表明,地方当局应仔细审视他们如何制定个人决定,并提高对服务应提供多长时间的认识。