Lankenau Medical Center and Institute for Medical Research, Wynnewood, PA
Riddle Hospital, Media, PA.
J Am Heart Assoc. 2017 Sep 22;6(9):e006508. doi: 10.1161/JAHA.117.006508.
Current guidelines recommend early P2Y inhibitor administration in non-ST-elevation myocardial infarction, but it is unclear if precatheterization use is associated with longer delays to coronary artery bypass grafting (CABG) or higher risk of post-CABG bleeding and transfusion. This study examines the patterns and outcomes of precatheterization P2Y inhibitor use in non-ST-elevation myocardial infarction patients who undergo CABG.
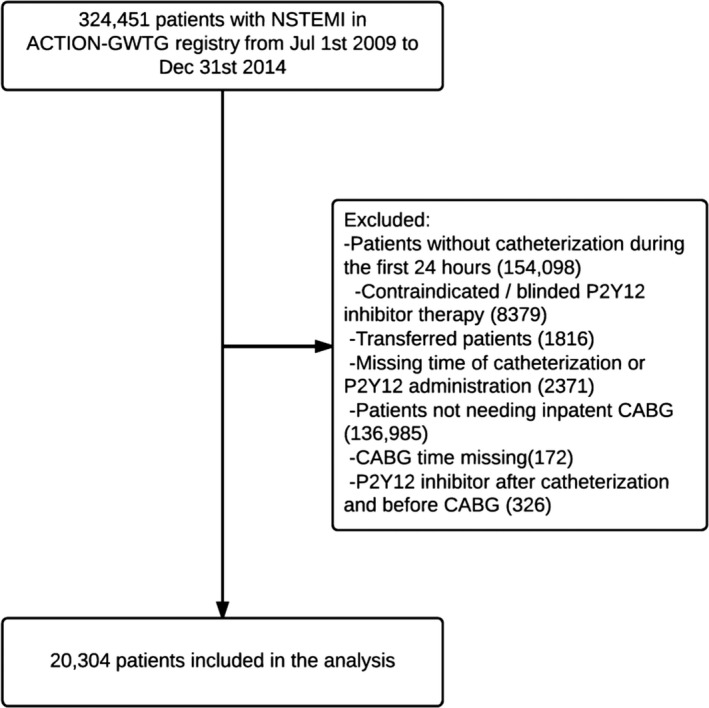
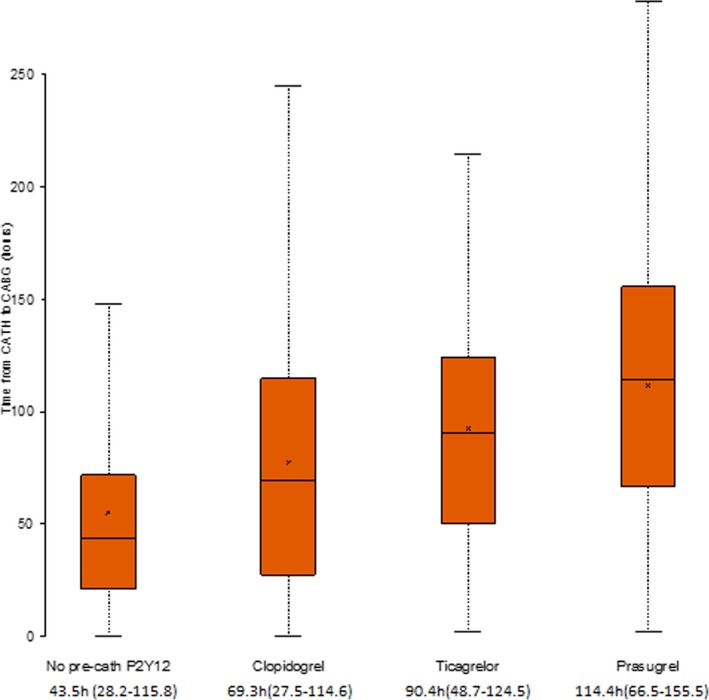
Retrospective analysis was done of 20 304 non-ST-elevation myocardial infarction patients in the ACTION (Acute Coronary Treatment and Intervention Outcomes Network) Registry (2009-2014) who underwent catheterization within 24 hours of admission and CABG during the index hospitalization. Using inverse probability-weighted propensity adjustment, we compared time from catheterization to CABG, post-CABG bleeding, and transfusion rates between patients who did and did not receive precatheterization P2Y inhibitors. Among study patients, 32.9% received a precatheterization P2Y inhibitor (of these, 2.2% were given ticagrelor and 3.7% prasugrel). Time from catheterization to CABG was longer among patients who received precatheterization P2Y inhibitor (median 69.9 hours [25th, 75th percentiles 28.2, 115.8] versus 43.5 hours [21.0, 71.8], <0.0001), longer for patients treated with prasugrel (median 114.4 hours [66.5, 155.5]) or ticagrelor (90.4 hours [48.7, 124.5]) compared with clopidogrel (69.3 [27.5, 114.6], <0.0001). Precatheterization P2Y inhibitor use was associated with a higher risk of post-CABG major bleeding (75.7% versus 73.4%, adjusted odds ratio 1.33, 95% confidence interval 1.22-1.45, <0.0001) and transfusion (47.6% versus 35.7%, adjusted odds ratio 1.51, 95% confidence interval 1.41-1.62, <0001); these relationships did not differ among patients treated with clopidogrel, prasugrel, or ticagrelor.
Precatheterization P2Y inhibitor use occurs commonly among non-ST-elevation myocardial infarction patients who undergo early catheterization and in-hospital CABG. Despite longer delays to surgery, the majority of pretreated patients proceed to CABG <3 days postcatheterization. Precatheterization P2Y inhibitor use is associated with higher risks of postoperative bleeding and transfusion.
目前的指南建议在非 ST 段抬高型心肌梗死患者中早期使用 P2Y 抑制剂,但尚不清楚经皮冠状动脉介入治疗前使用是否与冠状动脉旁路移植术(CABG)的延迟时间更长或 CABG 后出血和输血的风险更高有关。本研究旨在探讨接受 CABG 的非 ST 段抬高型心肌梗死患者经皮冠状动脉介入治疗前使用 P2Y 抑制剂的模式和结局。
对 ACTION(急性冠状动脉治疗和干预结果网络)登记处(2009-2014 年)的 20304 名非 ST 段抬高型心肌梗死患者进行了回顾性分析,这些患者在入院后 24 小时内行导管检查,并在住院期间接受 CABG。通过逆概率加权倾向调整,我们比较了接受和未接受经皮冠状动脉介入治疗前 P2Y 抑制剂治疗的患者之间从导管检查到 CABG 的时间、CABG 后出血和输血的发生率。在研究患者中,32.9%接受了经皮冠状动脉介入治疗前 P2Y 抑制剂治疗(其中 2.2%给予替卡格雷,3.7%给予普拉格雷)。与接受经皮冠状动脉介入治疗前 P2Y 抑制剂治疗的患者相比,接受经皮冠状动脉介入治疗前 P2Y 抑制剂治疗的患者从导管检查到 CABG 的时间更长(中位数 69.9 小时[25 百分位数,75 百分位数 28.2,115.8]比 43.5 小时[21.0,71.8],<0.0001),接受普拉格雷(中位数 114.4 小时[66.5,155.5])或替卡格雷(90.4 小时[48.7,124.5])治疗的患者比接受氯吡格雷(中位数 69.3 小时[27.5,114.6])的时间更长(<0.0001)。与未接受经皮冠状动脉介入治疗前 P2Y 抑制剂治疗的患者相比,接受经皮冠状动脉介入治疗前 P2Y 抑制剂治疗与 CABG 后大出血(75.7%比 73.4%,调整后的优势比 1.33,95%置信区间 1.22-1.45,<0.0001)和输血(47.6%比 35.7%,调整后的优势比 1.51,95%置信区间 1.41-1.62,<0.0001)的风险增加相关;在接受氯吡格雷、普拉格雷或替卡格雷治疗的患者中,这些关系没有差异。
在非 ST 段抬高型心肌梗死患者中,经皮冠状动脉介入治疗前使用 P2Y 抑制剂很常见,这些患者接受早期导管检查和院内 CABG。尽管手术延迟时间较长,但大多数经预处理的患者在经皮冠状动脉介入治疗后 <3 天内仍可进行 CABG。经皮冠状动脉介入治疗前使用 P2Y 抑制剂与术后出血和输血风险增加有关。