Schuller Bradley W, Burns Angi, Ceilley Elizabeth A, King Alan, LeTourneau Joan, Markovic Alexander, Sterkel Lynda, Taplin Brigid, Wanner Jennifer, Albert Jeffrey M
Department of Radiation Oncology, McKee Medical Center, Banner Health, Loveland, CO, USA.
J Appl Clin Med Phys. 2017 Nov;18(6):258-267. doi: 10.1002/acm2.12190. Epub 2017 Sep 25.
To report our early experiences with failure mode and effects analysis (FMEA) in a community practice setting.
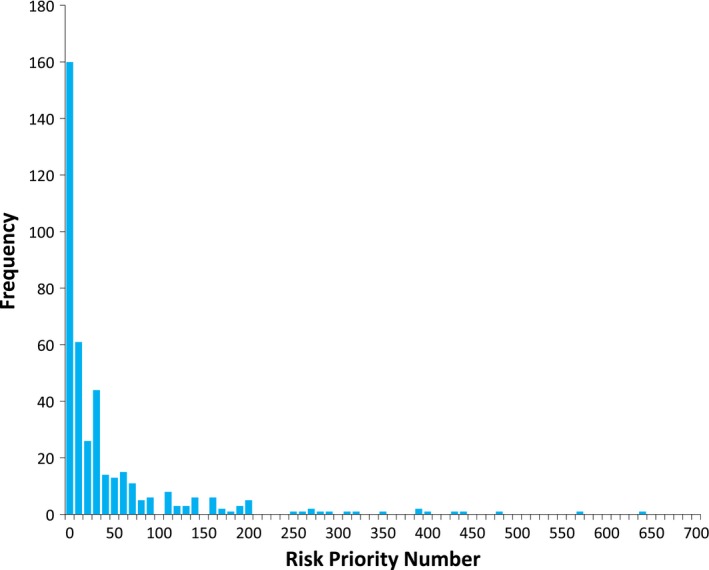
The FMEA facilitator received extensive training at the AAPM Summer School. Early efforts focused on department education and emphasized the need for process evaluation in the context of high profile radiation therapy accidents. A multidisciplinary team was assembled with representation from each of the major department disciplines. Stereotactic radiosurgery (SRS) was identified as the most appropriate treatment technique for the first FMEA evaluation, as it is largely self-contained and has the potential to produce high impact failure modes. Process mapping was completed using breakout sessions, and then compiled into a simple electronic format. Weekly sessions were used to complete the FMEA evaluation. Risk priority number (RPN) values > 100 or severity scores of 9 or 10 were considered high risk. The overall time commitment was also tracked.
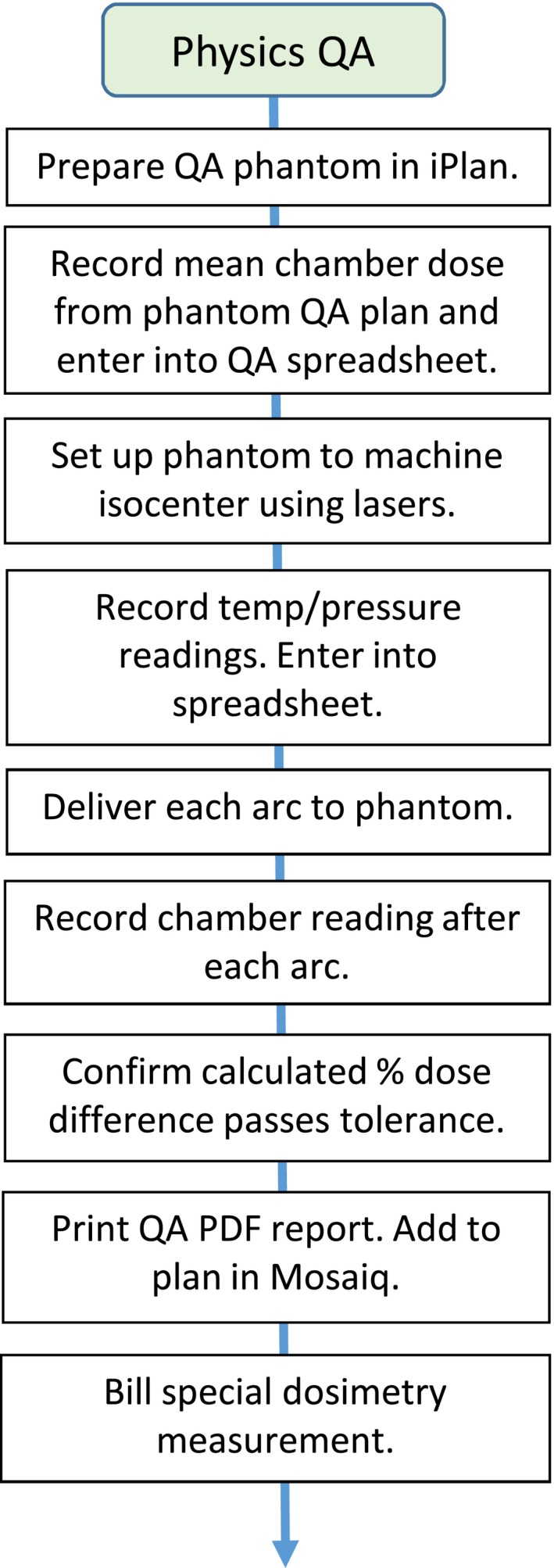
The final SRS process map contained 15 major process steps and 183 subprocess steps. Splitting the process map into individual assignments was a successful strategy for our group. The process map was designed to contain enough detail such that another radiation oncology team would be able to perform our procedures. Continuous facilitator involvement helped maintain consistent scoring during FMEA. Practice changes were made responding to the highest RPN scores, and new resulting RPN scores were below our high-risk threshold. The estimated person-hour equivalent for project completion was 258 hr.
This report provides important details on the initial steps we took to complete our first FMEA, providing guidance for community practices seeking to incorporate this process into their quality assurance (QA) program. Determining the feasibility of implementing complex QA processes into different practice settings will take on increasing significance as the field of radiation oncology transitions into the new TG-100 QA paradigm.
报告我们在社区实践环境中开展失效模式与效应分析(FMEA)的早期经验。
FMEA协调员在AAPM暑期学校接受了广泛培训。早期工作重点是部门教育,并强调在备受瞩目的放射治疗事故背景下进行流程评估的必要性。组建了一个多学科团队,成员来自各主要部门学科。立体定向放射外科(SRS)被确定为首次FMEA评估最合适的治疗技术,因为它在很大程度上自成体系,并且有可能产生高影响的失效模式。通过分组讨论完成流程映射,然后编制成简单的电子格式。每周进行会议以完成FMEA评估。风险优先数(RPN)值>100或严重程度评分为9或10被视为高风险。还跟踪了总体时间投入。
最终的SRS流程映射包含15个主要流程步骤和183个子流程步骤。将流程映射拆分为单独任务对我们的团队来说是一种成功策略。流程映射设计得包含足够细节,以便另一个放射肿瘤学团队能够执行我们的程序。协调员的持续参与有助于在FMEA期间保持评分一致。根据最高RPN分数进行了实践更改,新产生的RPN分数低于我们的高风险阈值。项目完成的估计人时当量为258小时。
本报告提供了我们完成首次FMEA所采取的初始步骤的重要细节,为寻求将此流程纳入其质量保证(QA)计划的社区实践提供了指导。随着放射肿瘤学领域向新的TG - 100 QA范式转变,确定在不同实践环境中实施复杂QA流程的可行性将变得越来越重要。