Shayesteh Moghaddam Narges, Jahadakbar Ahmadreza, Amerinatanzi Amirhesam, Skoracki Roman, Miller Michael, Dean David, Elahinia Mohammad
Dynamic and Smart Systems Laboratory, The University of Toledo, Toledo, OH 43606, USA.
Department of Plastic Surgery, The Ohio State University, Columbus, OH 43210, USA.
Bioengineering (Basel). 2017 Jan 22;4(1):5. doi: 10.3390/bioengineering4010005.
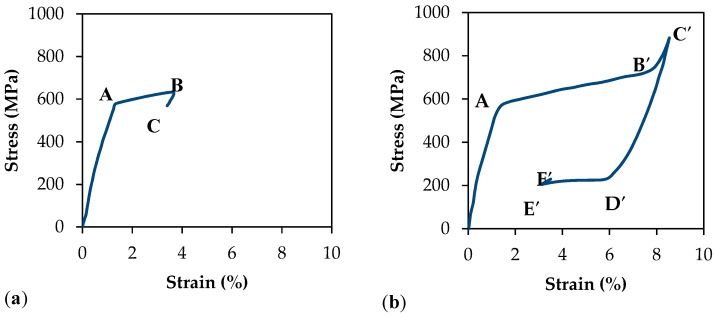
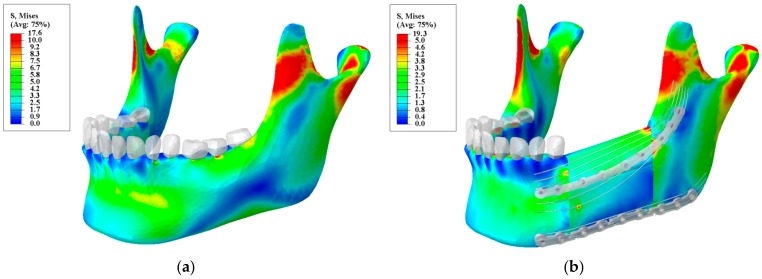
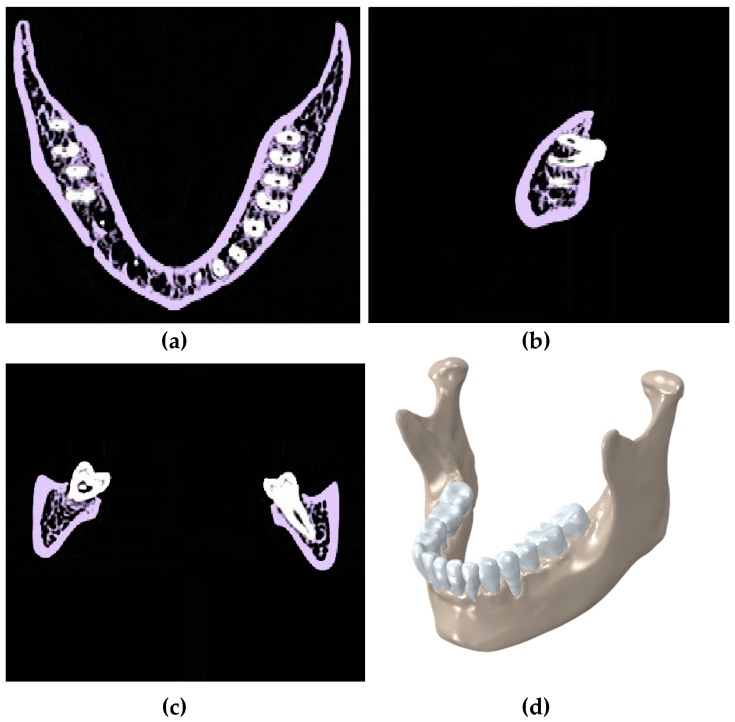
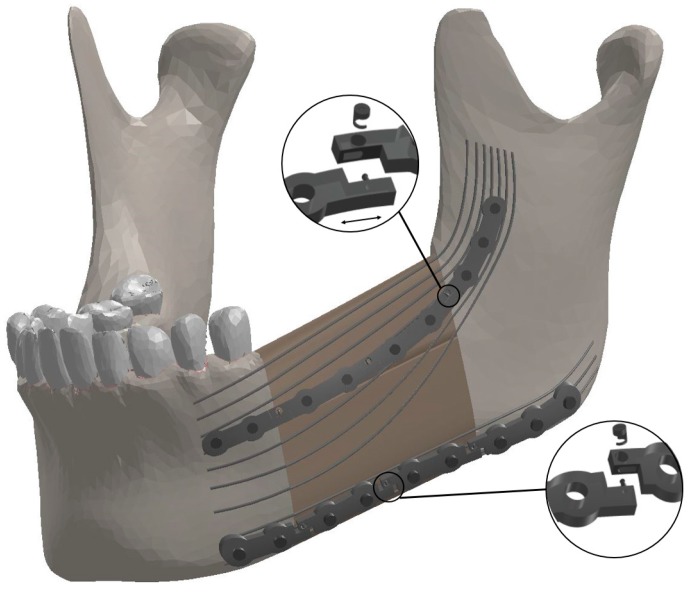
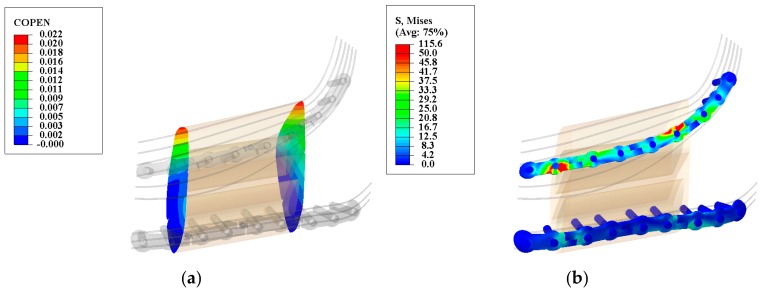
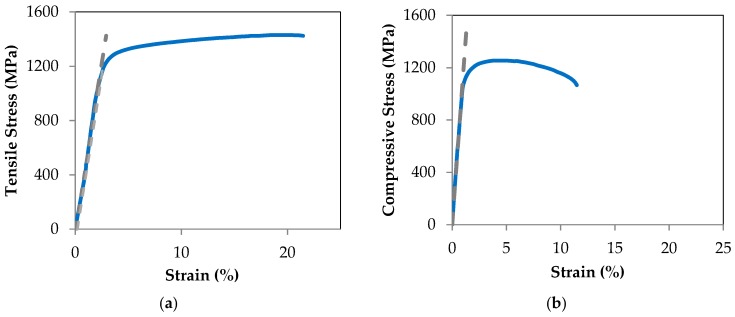
The current gold standard of care for mandibular segmental defeat reconstruction is the use of Ti-6Al-4V immobilization hardware and fibular double barrel graft. This method is often successful immediately at restoring mandible function, however the highly stiff fixation hardware causes stress shielding of the grafted bone and stress concentration in the fixation device over time which can lead to fixation device failure and revision surgery. The purpose of reconstructive surgery could be to create normal stress trajectories in the mandible following engraftment. We investigate the use of a two stage mechanism which separates the immobilization/healing and regenerative phases of mandibular segmental defect treatment. The device includes the use of a very stiff, Ti-6Al-4V, releasable mechanism which assures bone healing. Therefore it could be released once the reconstructed boney tissue and any of its ligamentous attachments have completely healed. Underneath the released Ti-6Al-4V plate would be a pre-loaded nitinol (NiTi) wire-frame apparatus that facilitates the normal stress-strain trajectory through the engrafted bone after the graft is healed in place and the Ti-6Al-4V fixation device has been released. Due to the use of NiTi wires forming a netting that connects vascularized bone and possibly bone chips, bone grafts are also more likely to be incorporate rather than to resorb. We first evaluated a healthy adult mandible during normal mastication to obtain the normal stress-strain distribution. Then, we developed the finite element (FE) model of the mandibular reconstruction (in the M1-3 region) with the proposed fixation device during the healing (locked state) and post-healing (released state) periods. To recreate normal stress trajectory in the reconstructed mandible, we applied the Response Surface Methodology (RMS) to optimize the Bone Bandaid geometry (i.e., wire diameters and location). The results demonstrate that the proposed mechanism immobilizes the grafted bone in the locked state properly since the maximum resultant gap (21.54 micron) between the graft and host mandible surfaces are in the safe region (less than 300 micron). By considering the von Mises criteria for failure, FE analysis together with experimental studies (i.e., compressive and tensile testing on the inferior and superior fixation devices, respectively) confirm that the proposed fixation devices do not fail, showing safety factor of at least 10.3. Based on the Response Surface Methodology (RSM) technique, the optimal parameter values for the wires are achieved (0.65 mm and 1 mm for the superior and inferior wires, respectively) and the required level of preload on each wire are calculated (369.8 N and 229 N for the inferior and superior wires, respectively). The FE results for stress distribution on the reconstructed mandible during the released state closely match that of a healthy mandible.
目前下颌骨节段性缺损重建的护理金标准是使用Ti-6Al-4V固定硬件和腓骨双筒移植。这种方法通常能立即成功恢复下颌骨功能,然而,随着时间的推移,高刚性的固定硬件会导致移植骨的应力遮挡和固定装置中的应力集中,这可能导致固定装置失效和翻修手术。重建手术的目的可能是在植入后在下颌骨中创建正常的应力轨迹。我们研究了一种两阶段机制的应用,该机制将下颌骨节段性缺损治疗的固定/愈合阶段和再生阶段分开。该装置包括使用一种非常刚性的Ti-6Al-4V可释放机制,以确保骨愈合。因此,一旦重建的骨组织及其任何韧带附着完全愈合,它就可以被释放。在释放的Ti-6Al-4V板下方将是一个预加载的镍钛诺(NiTi)线框装置,在移植骨在原位愈合且Ti-6Al-4V固定装置被释放后,该装置有助于通过植入骨的正常应力-应变轨迹。由于使用了形成连接血管化骨和可能的骨碎片的网的NiTi线,骨移植也更有可能被整合而不是吸收。我们首先评估了健康成年下颌骨在正常咀嚼过程中的正常应力-应变分布。然后,我们建立了下颌骨重建(M1-3区域)的有限元(FE)模型,该模型采用了所提出的固定装置,分别模拟愈合期(锁定状态)和愈合后期(释放状态)。为了在重建的下颌骨中重新创建正常的应力轨迹,我们应用响应面方法(RMS)来优化骨创可贴的几何形状(即线径和位置)。结果表明,所提出的机制在锁定状态下能正确地固定移植骨,因为移植骨与宿主下颌骨表面之间的最大合成间隙(21.54微米)处于安全区域(小于300微米)。通过考虑冯·米塞斯失效准则,有限元分析与实验研究(即分别对上下固定装置进行压缩和拉伸测试)一起证实,所提出的固定装置不会失效,安全系数至少为10.3。基于响应面方法(RSM)技术,获得了线的最佳参数值(上、下线分别为0.65毫米和1毫米),并计算了每根线上所需的预加载水平(下线和上线分别为369.8牛和229牛)。释放状态下重建下颌骨应力分布的有限元结果与健康下颌骨的结果紧密匹配。