Jeong Hye-In, Song Jinyoung, Choi Eun Young, Kim Sung Ho, Huh Jun, Kang I-Seok, Yang Ji Hyuk, Jun Tae Gook
Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Department of Pediatrics, Sejong General Hospital, Bucheon, Korea.
Korean Circ J. 2017 Sep;47(5):786-793. doi: 10.4070/kcj.2017.0033. Epub 2017 Sep 11.
We investigated the effectiveness of balloon dilatation of homograft conduits in the pulmonary position in delaying surgical replacement.
We reviewed the medical records of patients who underwent balloon dilatation of their homograft in the pulmonary position from 2001 to 2015. The pressure gradient and ratio of right ventricular pressure were measured before and after the procedure. The primary goal of this study was to evaluate the parameters associated with the interval to next surgical or catheter intervention.
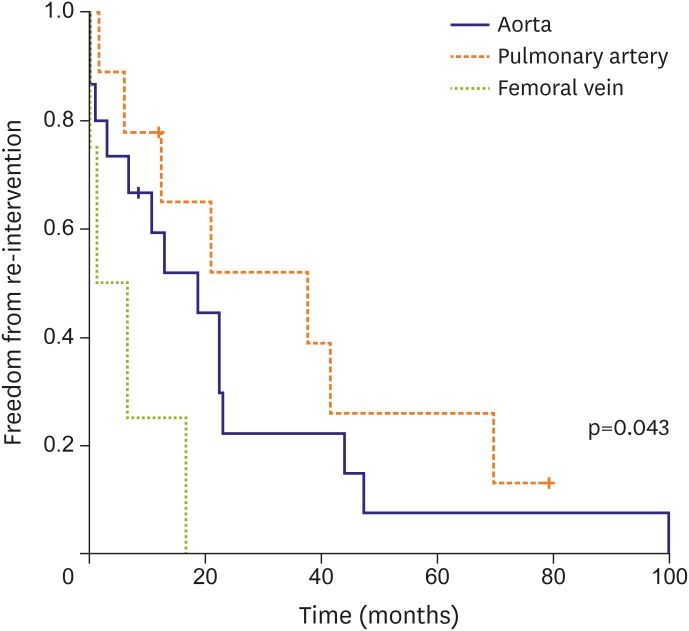
Twenty-eight balloon dilations were performed in 26 patients. The median ages of patients with homograft insertion and balloon dilatation were 20.3 months and 4.5 years, respectively. The origins of the homografts were the aorta (53.6%), pulmonary artery (32.1%), and femoral vein (14.3%). The median interval after conduit implantation was 26.7 months. The mean ratio of balloon to graft size was 0.87. The pressure gradient through the homograft and the ratio of right ventricle to aorta pressure were significantly improved after balloon dilatation (p<0.001). There were no adverse events during the procedure with the exception of one case of balloon rupture. The median interval to next intervention was 12.9 months. The median interval of freedom from re-intervention was 16.6 months. Cox proportional hazards analysis revealed that the interval of freedom from re-intervention differed only according to origin of the homograft (p=0.032), with the pulmonary artery having the longest interval of freedom from re-intervention (p=0.043).
Balloon dilatation of homografts in the pulmonary position can be safely performed, and homografts of the pulmonary artery are associated with a longer interval to re-intervention.
我们研究了肺动脉位同种异体移植物球囊扩张术在延迟手术置换方面的有效性。
我们回顾了2001年至2015年接受肺动脉位同种异体移植物球囊扩张术患者的病历。在手术前后测量压力梯度和右心室压力比值。本研究的主要目的是评估与下次手术或导管介入间隔相关的参数。
对26例患者进行了28次球囊扩张术。同种异体移植物植入和球囊扩张患者的中位年龄分别为20.3个月和4.5岁。同种异体移植物的来源为主动脉(53.6%)、肺动脉(32.1%)和股静脉(14.3%)。导管植入后的中位间隔时间为26.7个月。球囊与移植物大小的平均比值为0.87。球囊扩张术后,通过同种异体移植物的压力梯度以及右心室与主动脉压力比值显著改善(p<0.001)。除1例球囊破裂外,手术过程中未发生不良事件。下次干预的中位间隔时间为12.9个月。无再次干预的中位间隔时间为16.6个月。Cox比例风险分析显示,无再次干预的间隔时间仅因同种异体移植物的来源不同而有所差异(p=0.032),肺动脉来源的同种异体移植物无再次干预的间隔时间最长(p=0.043)。
肺动脉位同种异体移植物球囊扩张术可安全实施,肺动脉来源的同种异体移植物再次干预间隔时间更长。