Center for Multicultural Mental Health Research, Cambridge Health Alliance & Harvard Medical School, Cambridge, MA, USA.
Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA.
Depress Anxiety. 2017 Dec;34(12):1147-1156. doi: 10.1002/da.22681. Epub 2017 Sep 29.
The Food and Drug Administration's 2004 antidepressant warning was followed by decreases in antidepressant prescribing for youth. This was due to declines in all types of depression treatment, not just the intended changes in antidepressant prescribing patterns. Little is known about how these patterns varied by race/ethnicity.
Data are Medicaid claims from four U.S. states (2002-2009) for youth ages 5-17. Interrupted time series analyses measured changes due to the warning in levels and trends, by race/ethnicity, of three outcomes: antidepressant prescription fills, depression treatment visits, and incident fluoxetine prescription fills.
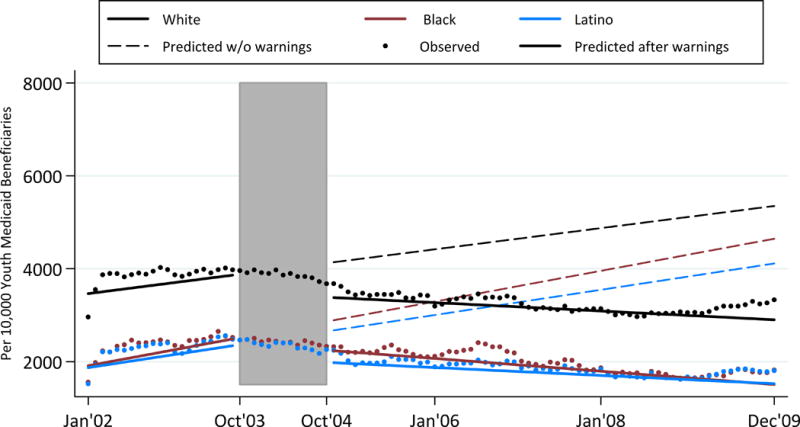
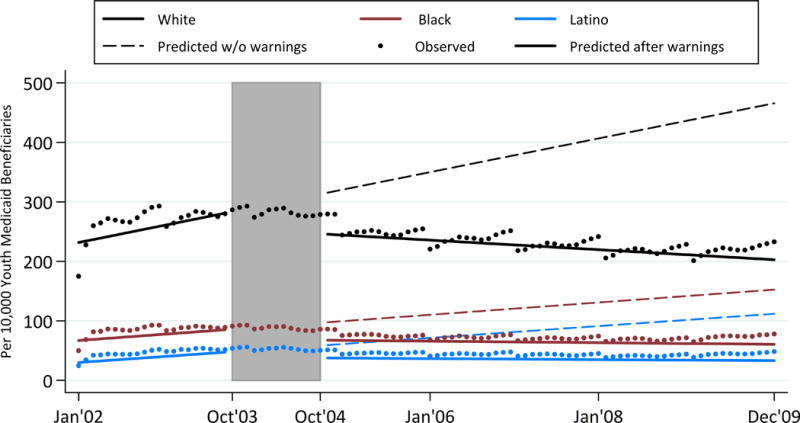
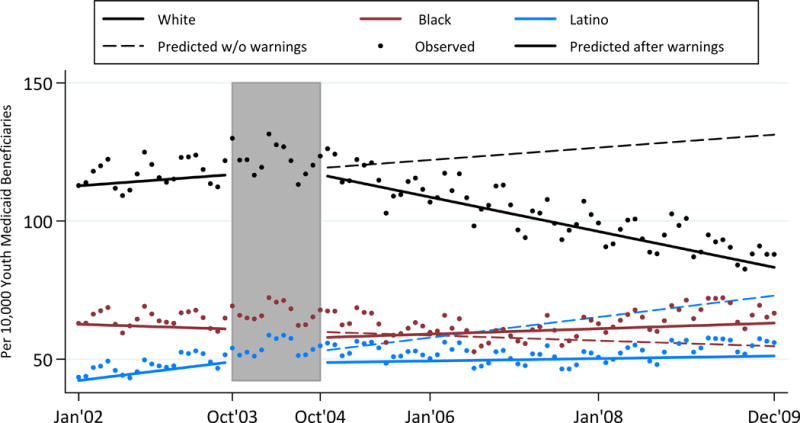
Prewarning, antidepressant fills were increasing across all racial/ethnic groups, fastest for White youth. Postwarning, there was an immediate drop and continued decline in the rate of fills among White youth, more than double the decline in the rate among Black and Latino youth. Prewarning, depression treatment visits were increasing for White and Latino youth. Postwarning, depression treatment stabilized among Latinos, but declined among White youth. Prewarning, incident fluoxetine fills were increasing for all groups. Postwarning, immediate increases and increasing trends of fluoxetine fills were identified for all groups.
Antidepressant prescription fills declined most postwarning for White youth, suggesting that risk information may have diffused less rapidly to prescribers or caregivers of minorities. Decreases in depression treatment visits help to explain the declines in antidepressant prescribing and were largest for White youth. An increase in incident fluoxetine fills, the only medication indicated for pediatric depression at the time, suggests that the warning may have shifted prescribing practices.
美国食品和药物管理局 2004 年的抗抑郁药警告发布后,青少年的抗抑郁药处方量有所减少。这是由于所有类型的抑郁症治疗都有所减少,而不仅仅是抗抑郁药处方模式的预期变化。对于这些模式如何因种族/族裔而异,知之甚少。
数据来自美国四个州的医疗补助计划(2002-2009 年)的青年(5-17 岁)的医疗记录。中断时间序列分析衡量了警告对三种结果(抗抑郁药处方数量、抑郁症治疗就诊次数和氟西汀处方数量)的水平和趋势变化,按种族/族裔进行分组。
在预警之前,所有种族/族裔群体的抗抑郁药用量都在增加,白人青少年的增长速度最快。在预警之后,白人青少年的抗抑郁药用量立即下降,并持续下降,降幅是黑人和拉丁裔青少年的两倍多。在预警之前,白人青少年和拉丁裔青少年的抑郁症治疗就诊次数都在增加。在预警之后,拉丁裔青少年的抑郁症治疗稳定下来,但白人青少年的治疗却下降了。在预警之前,所有群体的氟西汀用量都在增加。在预警之后,所有群体的氟西汀用量都立即增加,且呈上升趋势。
抗抑郁药处方用量在预警后下降最多的是白人青少年,这表明风险信息可能向少数族裔的医生或照顾者传播得较慢。抑郁症治疗就诊次数的减少有助于解释抗抑郁药处方量的减少,而且这种减少在白人青少年中最大。氟西汀用量的增加(当时唯一被批准用于儿童抑郁症的药物)表明,该警告可能改变了处方实践。