Santos E M M, d'Esterre C D, Treurniet K M, Niessen W J, Najm M, Goyal M, Demchuk A M, Majoie C B, Menon B K, Marquering H A
Department of Biomedical Engineering and Physics, Academic Medical Center, Amsterdam, The Netherlands.
Department of Medical Informatics, Erasmus Medical Center, Rotterdam, The Netherlands.
Neuroradiology. 2018 Jan;60(1):71-79. doi: 10.1007/s00234-017-1907-y. Epub 2017 Sep 30.
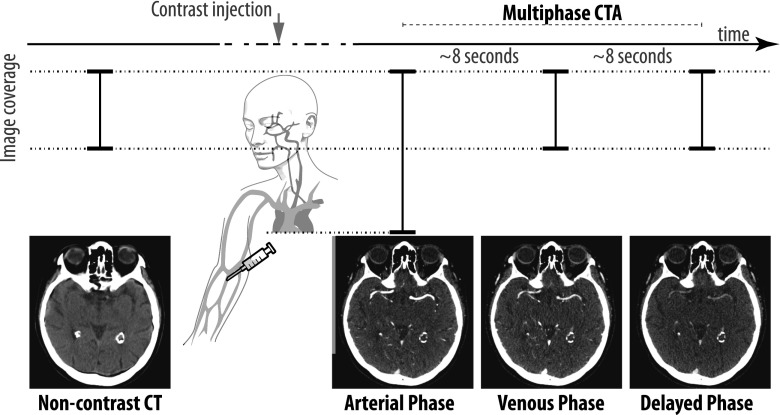
Thrombus perviousness has been associated with favorable functional outcome in acute ischemic stroke (AIS) patients. Measuring thrombus perviousness on CTA may be suboptimal due to potential delay in contrast agent arrival in occluded arteries at the moment of imaging. Dynamic sequences acquired over time can potentially overcome this issue. We investigate if dynamic CTA has added value in assessing thrombus perviousness.
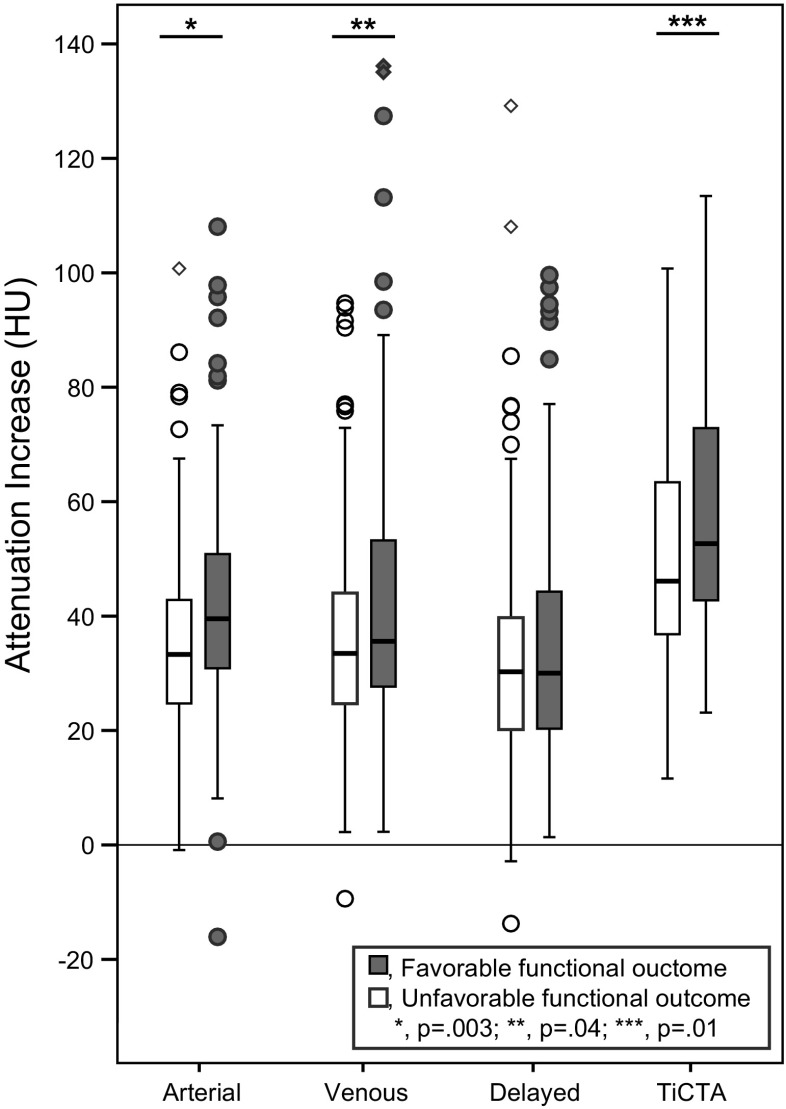
Prospectively collected image data of AIS patients with proven occlusion of the anterior or posterior circulation with thin-slice multi-phase CTA (MCTA) and non-contrast CT were co-registered (n = 221). Thrombus attenuation increase (TAI; a perviousness measure) was measured for the arterial, venous, and delayed phase of the MCTA and time-invariant CTAs (TiCTA). Associations with favorable clinical outcome (90-day mRS ≤ 2) were assessed using univariate and multivariable regressions and calculating areas under receiver operating curves (AUC).
TAI determined from the arterial phase CTA was superior in the association with favorable outcome with OR = 1.21 per 10 HU increase (95%CI 1.04-1.41, AUC 0.62, p = 0.014) compared to any other phase (venous 1.14(95%CI 1.01-1.30, AUC 0.58, p = 0.033), delayed 1.046(95%CI 0.919-1.19, AUC 0.53, p = 0.50)), and TiCTA (1.15(95%CI 1.02-1.30, AUC 0.60, p = 0.022). In the multivariable model, only TAI on arterial phase was significantly associated with favorable outcome (aOR 1.59, 95%CI 1.04-2.43, p = 0.032).
Association between TAI with functional outcome was optimal on arterial-phase CTA such that dynamic CTA imaging has no additional benefits in current thrombus perviousness assessment, thereby suggesting that the delay of contrast arrival at the clot is a key variable for patient functional outcome.
在急性缺血性卒中(AIS)患者中,血栓通透性与良好的功能预后相关。由于成像时造影剂到达闭塞动脉可能存在潜在延迟,因此在CTA上测量血栓通透性可能并不理想。随时间获取的动态序列可能会克服这一问题。我们研究动态CTA在评估血栓通透性方面是否具有附加价值。
前瞻性收集经证实存在前循环或后循环闭塞的AIS患者的图像数据,将薄层多期CTA(MCTA)和非增强CT进行配准(n = 221)。测量MCTA的动脉期、静脉期和延迟期以及时间不变CTA(TiCTA)的血栓衰减增加(TAI;一种通透性测量指标)。使用单变量和多变量回归以及计算受试者操作曲线下面积(AUC)来评估与良好临床结局(90天改良Rankin量表评分≤2)的相关性。
与其他任何时期相比,动脉期CTA确定的TAI与良好结局的相关性更佳,每增加10 HU的OR为1.21(95%CI 1.04 - 1.41,AUC 0.62,p = 0.014),静脉期为1.14(95%CI 1.01 - 1.30,AUC 0.58,p = 0.033),延迟期为1.046(95%CI 0.919 - 1.19,AUC 0.53,p = 0.50),TiCTA为1.15(95%CI 1.02 - 1.30,AUC 0.60,p = 0.022)。在多变量模型中,只有动脉期的TAI与良好结局显著相关(校正后OR 1.59,95%CI 1.04 - 2.43,p = 0.032)。
在动脉期CTA上,TAI与功能结局之间的相关性最佳,因此动态CTA成像在当前血栓通透性评估中没有额外益处,这表明造影剂到达血栓的延迟是影响患者功能结局的关键变量。